

Content Sections
By Rob Verkerk PhD, founder, executive and scientific director, ANH Intl
In the wake of the Better Way conference in Bath (UK), it’s been nothing short of mind-blowing sharing time over the last two weeks with fellow activists for better health systems, if that’s how we should refer to what we’re trying to co-create.
“Some may still want to choose a shackled life that is designed and determined in ivory towers and corporate board rooms, but let that be a choice, not our sole option."
— Rob Verkerk, PhD
With some irony, it is the orchestrated, global deception and broad mismanagement of SARS-CoV-2 by health authorities that has brought so many of us together – groups of people from diverse backgrounds, including doctors, other health practitioners, scientists, lawyers – along with millions of others around the world. People who wouldn’t have come together otherwise, or at least within such a compressed time frame. So with all the suffering that’s occurred, the unnecessary lives lost, the grief, the iatrogenically injured, the lost livelihoods, the social deprivation, and the shifting sands of power structures, we must still find some space for gratitude.
Thank you, covid-19 (C19), for being a catalyst for a revolution that was desperately needed, one that allows liberty, human creativity, hope and nature to conspire in ways that facilitate the future fitness of our species. Some may still want to choose a shackled life that is designed and determined in ivory towers and corporate board rooms, but let that be a choice, not our sole option.
With that said, I wanted to take you on a short journey that includes some of the reflections I’ve shared over the last few days with some of our international collaborators, all brought together under the umbrella of the World Council for Health. You’ll find short extracts of some of these reflections recorded in our offices in Chilworth (Surrey, UK), with Dr Naseeba Kathrada (South Africa), Dr Mark Trozzi (Canada), Rain Trozzi (Canada), Meleni and myself.
In this piece, I want to reflect specifically on three statistics that have dominated many minds and created huge polarisation depending on their interpretation.
These are:
- C19 deaths
- C19 cases, and
- vaccination adverse events.
Official figures on all three tend to be unreliable, spurious or are widely misrepresented or misinterpreted, and cannot be relied upon to understand the real impacts of C19 disease, as distinguished from the impacts of the human response, statistical noise or statistical manipulation.
Prof Norman Fenton and colleagues’ dismantling of official UK data of C19 injected and un-injected cases, previously widely regarded as the most reliable dataset available internationally, provided a stark reminder of how deception can work.
Reflecting on the dead
As painful as it might be for those of us who’ve lost loved ones over the last two years, it’s necessary to reflect on the mortality data associated with C19 if we’re not to see history repeated. Reported C19 deaths were always conflated with other causes, as, in the majority of countries, they always represented deaths reported from any cause that occurred within specified time frames (e.g. 28 days, 60 days) of a positive C19 antigen (usually PCR) test.
Many of these reported deaths were in hospitals where the sickest people tend to go, and hospitals were also among the most likely places to contract an infection, and certainly the most likely place to test for C19 status using a flawed diagnostic technique, based on the various C19 RT-PCR platforms.
So we’re left with no accurate way of measuring C19 disease impact accurately, just a proxy for C19 disease impact: a comparison of all-cause mortality against the expected average mortality, in other words so-called ‘excess mortality’.
Contrary to the views of some – there was an undeniable elevated excess mortality in some, but far from all, countries. These coincided with waves of apparent infection. To summarise: some countries, including almost all 55 countries of the African continent and around one-third of European countries, experienced no excess mortality wave whatsoever, while others experienced, one, two or three excess mortality waves of varying severity.
Using the comprehensive excess mortality dataset of the 28 EuroMOMO partners, including most EU countries, the UK nations and Israel, 9 (32%) experienced no significant excess mortality impact between 2020 to the present, namely; Cyprus, Denmark, Estonia, Finland, Greece, Luxembourg, Malta, Norway and Northern Ireland. You can see this for yourself by scanning the 'Z-scores by country' section at the bottom of the EuroMOMO graphs and maps page here.
There is no clear, strong positive or negative correlation between excess mortalities (or case rates) and C19 injection rates. Having said this, analysis of official data banked in Our World in Data shows that all the countries with the highest excess mortalities also tended to have among the highest rates of ‘full vaccination’. Again, using the EuroMOMO dataset by example, Belgium, France, Italy, the Netherlands, Spain and the UK suffered the highest peaks of excess mortality in Europe and these coincided with infection waves as determined by antigen testing and hospitalisations. These countries all had among the highest rates of injection, varying between 78% and 88% (Fig. 1), however there are insufficient data to determine if vaccination is causally associated with excess mortality or otherwise.
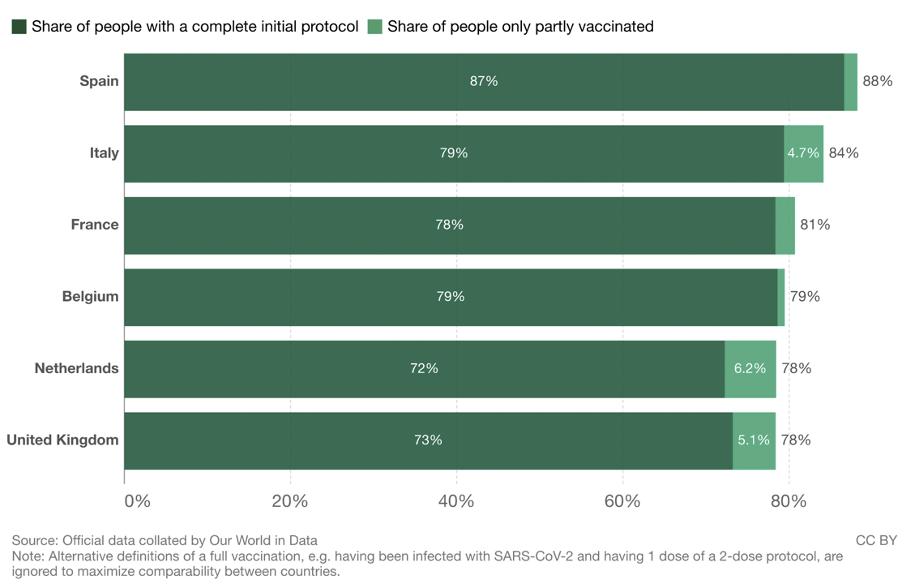
Figure 1. Share of people in European countries with highest excess mortalities who have received C19 injections. Source: Our World in Data.
Then we’ve got to try to unpick why there is increased excess mortality across all 28 EuroMOMO partner countries in 2021, compared with 2020, in all age groups between 15 and 74 (Fig. 2). How much of this was mortality induced by C19, and how much was caused by the breakdown of primary and secondary health care services during the ‘pandemic’? But could the vaccines have played a part as well? It would be foolish to ignore this possibility given that the excess mortality in progressively younger age groups is delayed, as was the roll-out of C19 ‘vaccines’ (Fig. 2).
You'll also notice there is a pronounced increase in excess mortality in the 0-14 year group (Fig. 2, top) in 2021 compared with 2020, this kicking in around week 38 (the third week of September 2021) when C19 injections were being encouraged in adolescents. European roll-out of lower doses for 5 to 11-year-olds started in December 2021. But there are insufficient data to relate any of this speculation causally to the C19 injections, or to properly understand the relative importance of the different factors that contributed to this mortality.
It is nonetheless reassuring that excess mortalities for 2022 are tracking lower than 2021 (Fig. 2), and this may be linked to the declining deadliness of SARS-CoV-2 infection, lower C19 ‘vaccine’ uptake and the partial restoration of primary and secondary care services.
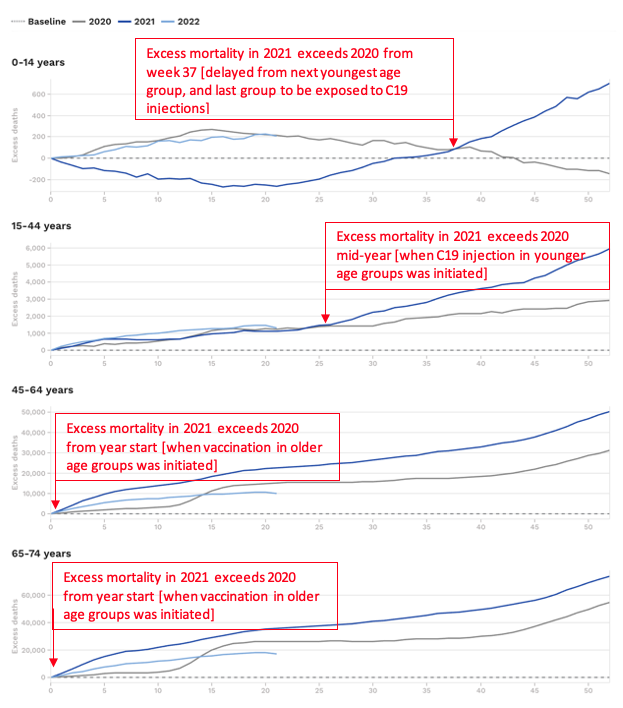
Figure 2. Excess mortalities among 28 EuroMOMO partner countries among 4 age groups showing delay in raised excess mortalities in 2021 compared with 2021 in youngest two age groups. Source: EuroMOMO.
We can also look at the US data, courtesy of the US Centers of Disease Control and Prevention (CDC) (Fig. 3).
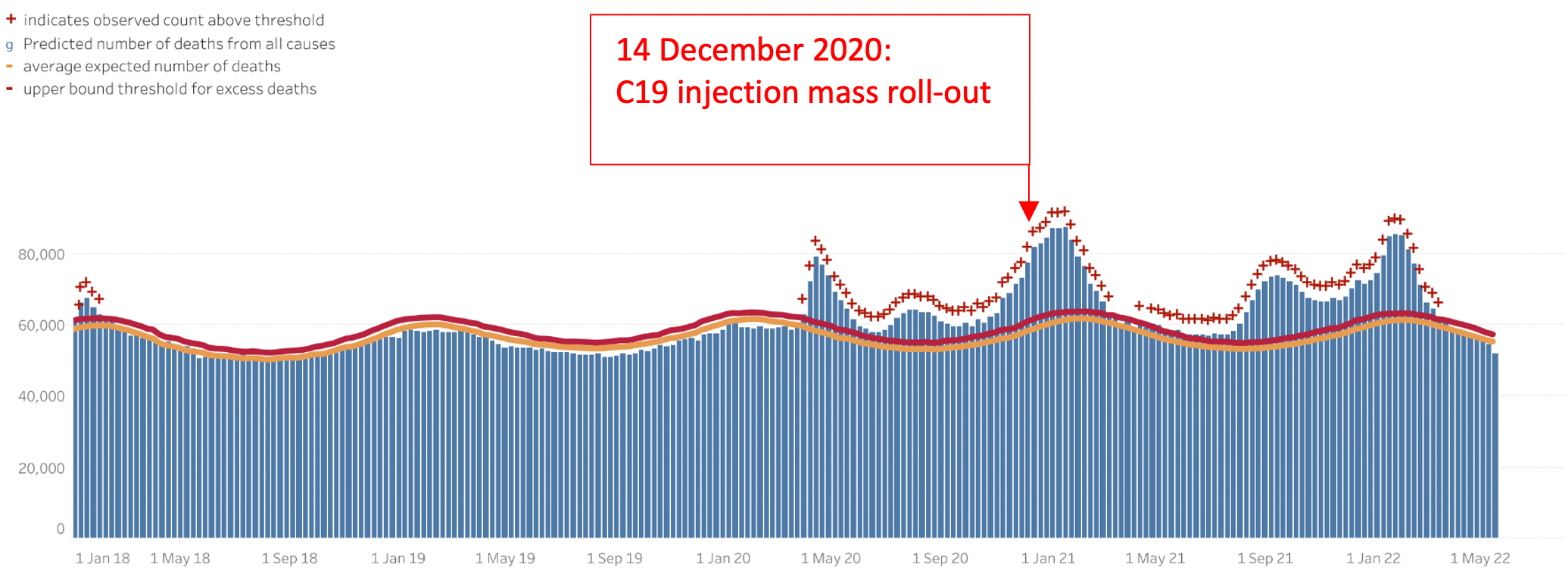
Figure 3. Excess mortalities in the USA from January 2018 to May 2022. Source: CDC.
Anyone who continues to broadcast the idea that C19 ‘vaccination’ saved the day should look more closely at these data. Vaccination is intended to stop community transmission and this just hasn’t happened. Nor did deaths drop following vaccination despite successive variants losing pathogenic strength and authorities claiming the vaccines were protecting people from severe disease and death. The net excess mortality post-C19 injection roll-out actually considerably exceeds that of the pre-rollout period (note area under the curves before and after roll-out) — when the virulence of the early viral variants was considerably greater and naturally-acquired immunity much lower.
In fact it was these two factors that yielded the short sharp excess mortality peaks for the first wave, this being explained to a large part by a 'dry tinder' effect in which older, vulnerable people with comorbidities were taken out quickly and prematurely, rather than these deaths being more spread out in time.
It would be premature to imagine that C19 will no longer be part of our lives given the virus is still at large, with an ability to mutate and become either more virulent (deadly), transmissible (contagious) – or both. Made all the more likely if selection pressure from ongoing C19 vaccines is maintained in large sectors of the global population.
And we're a long way from authorities withdrawing the intense coercion to force people, especially those who have consistently resisted, into using genetic vaccines that have delivered marginal benefit and extensive, yet greatly under-reported, harms.
Cases defined by PCR test
The second statistic we must take with a pinch of salt is case data. These data are afflicted with several important methodological problems, including:
- RT-PCR tests were rolled out globally with no gold standard meaning there was no accurate way of determining the positive predictive value of the many different testing platforms used as the primary diagnostic method
- Initial case data were based on PCR tests that were classified as positive sometimes with well over 30 amplification cycles (cycle threshold, CT). Such tests with high CT values (>28) typically measure RNA fragments that are not from ‘live’ virus that can replicate and cause C19 disease. Different testing authorities and countries imposed limits on CTs at different times so evaluating case data throughout the two plus years of the ‘pandemic’ period is like comparing apples with oranges. Given CT is inversely proportional to viral load, a much better and more accurate picture of disease status in space and time could have been revealed had CT data also been shared widely where these data were available.
- PCR and related CT data should never be used in isolation from the clinical picture and history. Yet PCR was used as the primary diagnostic for C19 disease (while often ignoring other respiratory or other diseases) – for the first time in history, in the absence of assessments of clinical disease or pathology. Eliminating the gathering of information that helps the clinician build a picture of an individual’s clinical history and replacing it with genetic sequencing techniques for diagnosis could one day be seen as one of the gravest errors in medicine. It focuses people on a genetic pathogen or risk factor and ignores the importance of the environment, the terrain (‘constitution’) and epigenetics, that ultimately controls our genetic expression and phenotypic vehicle we're gifted with during our lifetimes.
- Any diagnostic disease yields more false positives when prevalence declines. This is a statistical artifact described by Bayes’ theorem and it is recognised by all health authorities (e.g. WHO here), yet it is rarely discussed or publicised. This artefact means that you can effectively have a never ending pandemic because as the prevalence drops close to zero, false positives increase giving the impression of increased disease prevalence.
C19 injection adverse events
The third statistic that we’ve all been looking at are reported adverse events associated with C19 injections. The OpenVAERS project summarises available, officially reported US adverse event data, including C19 injection related events and mortalities, very comprehensively (Figs 4 and 5).
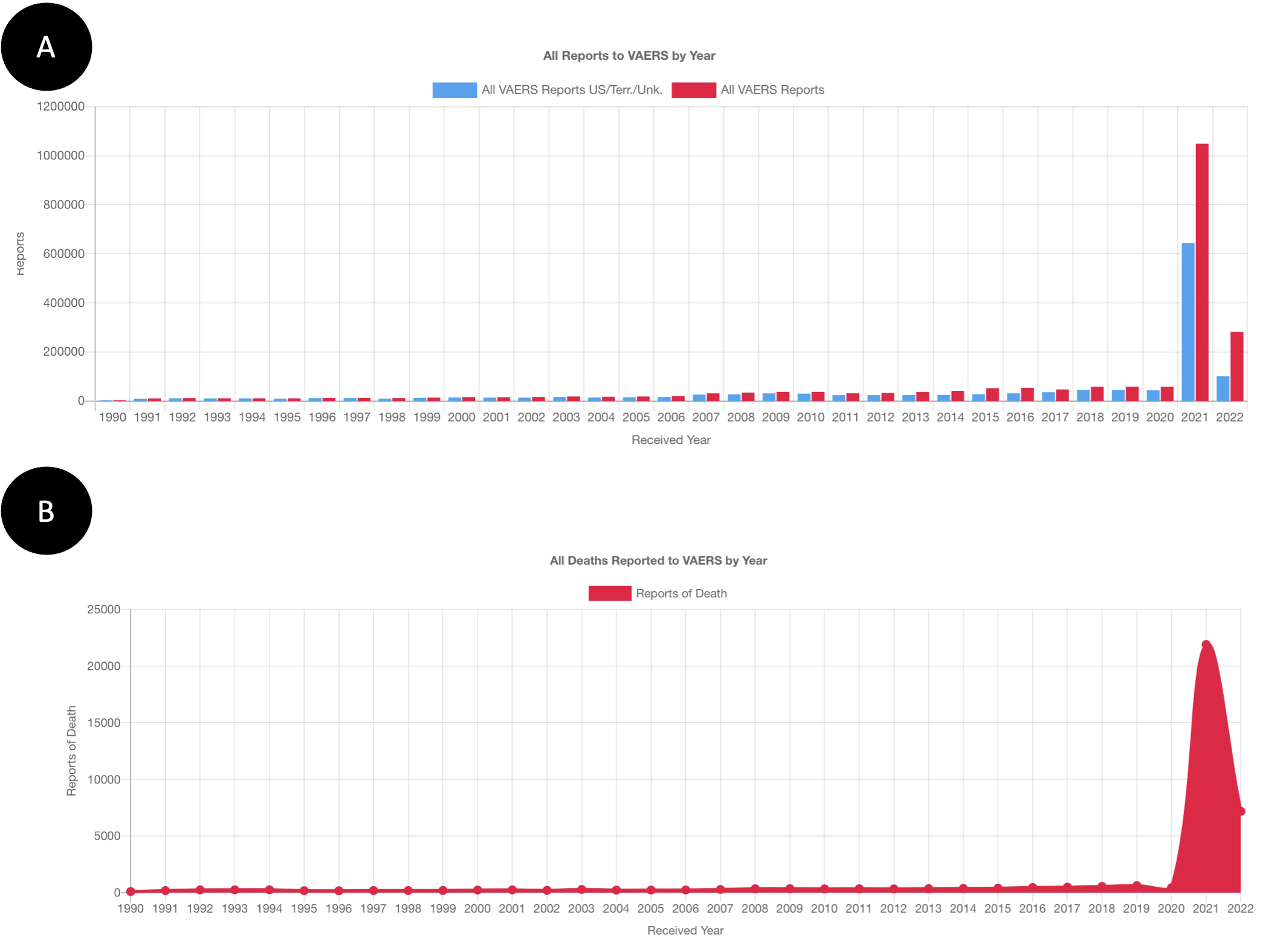
Figure 4. A: All reports to VAERS: 1990-May 2022. B: All deaths reported to VAERS: 1990-May 2022. Source OpenVAERS.
The uptick in 2020 for the biggest vaccination roll-out of largely experimental products in US history – as well as the largest experiment conducted on human populations in world history – in 2021 is revealing (Fig. 4). With almost five months of data received for 2022, it’s looking like VAERS reports this year won’t exceed those of 2021.
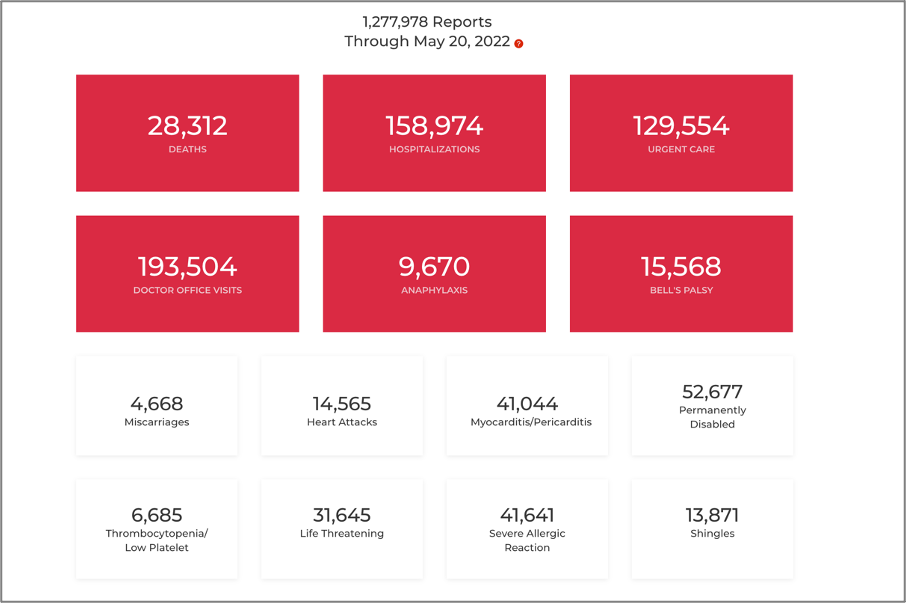
Figure 5. OpenVAERS ‘red box’ summaries through to 20 May 2022. Source: OpenVAERS.
But complacency would be obtuse. These statistics, as they stand currently, should be enough to make front page news. Instead, we continue to hear health authorities parrot the deception that C19 injections are “safe” (e.g. CDC here, NHS here).
>>> At this point, we’d like to ask any reader of this article who might be interested in co-funding a legal challenge against this deceptive advertising claim to contact us at [email protected] – or call our office (see contact details on our website)
Many people need reminding that each and every reported case is not easy to make. It requires a lot of time and patience, whether it’s a healthcare provider, a patient, a parent or a caregiver. The reporter also needs to be sufficiently convinced the event is related to the injection. In the recent climate of coercion and brainwashing, many cases go unreported. This might mean that reporting is even lower, potentially much lower, than the 1% underreporting for vaccines suggested by Harvard researchers investigating the VAERS system.
But what none of these reports are able to take into account is that adverse reactions triggered by one or chronic exposure to the injections might take months or even years to manifest or be recognised. Such as the fertility issues, the triggering of autoimmune conditions, the heart tissue scarring, or the damage to the brain and other parts of the neurological system. Or the consequences of disrupted immune function, suppression of T lymphocytes (T cell lymphopenia) from severe C19 disease or repeat vaccination that increases cancer risk or the recurrence of cancer following its remission.
As with excess mortality, we need to keep a close eye on prevalence of a very wide range of conditions and compare these in populations that have been highly C19 ‘vaccinated’ – and yes, against those C19 ‘unvaccinated’. Big shout out here to anyone who’s volunteered to remain in the control group.
And rather than castigating those doctors and other health practitioners that are awake to the seriousness of these C19 jab injuries, how about some gratitude, respect and support for this marginalised group who continue to be true to the Hippocratic oath that they’ve committed to. Whilst often facing witch-hunts, risking or losing their previous careers and sometimes even risking their personal safety.
Final reflections
These three statistics offer a tiny window into the maelstrom of the last two years that has variously been referred to as a pandemic, a plandemic, a crisis, the Great Reset (see here and here), an opportunity to consolidate global power, or the dawn of transhumanism.
I started out by offering gratitude for how these two years have brought together so many likeminded people with a deep mission to do something that will help rather than hinder humanity.
The ‘locus of trust’ for many people has changed dramatically. Corruption has been exposed, though rarely acted upon through the judiciary, such is the depth of corruption through all the major organs of society.
But, honestly, who would trust the majority of mainstream news media for accurate scientific or medical reporting after what we’ve experienced? Or the majority of health authorities, the machinery of which is deeply intertwined with the profit- and power-hungry government-pharmaceutical corporatocracy. When it comes to news, supply and demand being what it is, is already driving the creation of better, more objective, more balanced new media, with a plethora of actors. A new media that understands that paid-for science and conflicted scientists with vested interests are hardly going to provide a representative picture of what’s really going on or what we should do to protect ourselves and our communities.
Cheap natural treatments, such as vitamin D, vitamin C, zinc and quercetin, as well as a product originating from a humble soil-dwelling bacterium – ivermectin – were the clear winners over the billions spent on novel genetic injections.
Most of all, we’ve learned that many of us will stand shoulder to shoulder and find ways, regardless of the scale of the Goliath we face, to maintain sufficient frequency within our minds and bodies to not onboard approaches being thrust on us by the ruling authoritarians that simply don't make sense to our own and unique systems of values, principles and beliefs.
That's going to be a prerequisite for what's in store for us - because if you think we're now able to stroll through the post-covid plains into the sunset, think again - while reading what Ursula von der Leyen and others have in store for us after the northern hemisphere summer. The unvaccinated will remain the out-group, the scapegoat and the discrimination target for as long as the current ruling plutocracy remains all-powerful.
This is not the time to call fatigue, apathy or a sense of disempowerment. We have a choice to not engage in systems that would force us to compromise many of the fundamental rights and principles we consider to integral to civilised human societies - and while that can incur costs and hardship, non-engagement is a central to our win in this battle of hearts, minds and spirits.
In April 2020, I wrote a piece asking “Have we lost control to the state?” and I proposed we keep our eyes wide open.
Stay healthy, stay fit, stay resilient, and elevate your frequency as far as you can….and let’s open our eyes wider still.
>>> Footnote: Next month, we’re going to be running a soon-to-be-publicised event that will focus on how we can maintain psychological, emotional and spiritual resilience given the world we must now navigate. Stay tuned!
>>> Alliance for Natural Health International re-Publishing Guidelines
>>> Has this article generated questions for you? Did you know our ANH Pathfinder Members get a free monthly Q&A as part of their annual membership? Why not Join us!
>>> Visit covidzone.org for our full coverage of the coronavirus crisis and beyond
Proudly affiliated with: Enough Movement Founding coalition partner of: World Council for Health




Comments
your voice counts
There are currently no comments on this post.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences