

Content Sections
By Rob Verkerk PhD
Founder, executive and scientific director
Last week we rebutted a Spanish study that warned of high protein intake. This week, we dig deeper into proteins, probably the least well understood of the three macronutrient groups, which also include carbohydrates and fats. The two big questions we want to look at, neither of which we can expect to have absolute or definite answers to, are: what quality and how much protein do we need?
Protein basics
Proteins are molecules comprised of amino acids. Amino acids are in turn produced according to different nucleotide sequences in our DNA, these being variants of nucleotide triplets called codons that form the basis of our ‘genetic code’.
Proteins are involved in almost every process in the body, and have a vast array of essential functions. These include structural (e.g. collagen and elastin in skin, in nerve cells), mechanical (e.g. contractile proteins in muscle tissue) and immune (e.g. antibodies and cytokines in the immune system) functions. They act as catalysts for biochemical reactions (enzymes) and as transporters (e.g. haemoglobin for oxygen) and signalling compounds (e.g. cytokines, peptides, hormones). They can also serve as fuel, yielding around 4 calories (kcal) per gram, on par with carbohydrates, but less than half that of fats, which yield 9 calories per gram.
Proteins are the key functional molecules expressed by genes, in a two-step process, the first step being transcription, the second translation.
Depending on your background knowledge of science, some might find it useful to recap on the basics about what proteins are using this animation produced by the Genetic Science Learning Center at the University of Utah.
Amino acid sequences so produced as gene products can then be modified following translation, by the addition of different chemical groups (e.g. methyl, phosphate) that further alter their function in the body. Other gene regulator proteins can turn genes on or off, so coded proteins are produced only at specific times during an organism’s development or according to need. While the genetic code determines the protein sequence to be expressed in a given coding region of our chromosomes, other, more distant, parts of our genome can influence when and where proteins are expressed. This newer understanding of gene expression is an important reason for concerns about genetic engineering technology.
A small number of amino acids joined together are called peptides, bigger ones polypeptides and larger or longer polypeptides are referred to as proteins. Proteins also often undergo complex folding that also dictates their function.
Amino acids can be categorised according to their essentiality by the human body. Three groups are often distinguished (Table 1).
Table 1. Essential, conditionally essential and non-essential proteinogenic amino acids in humans
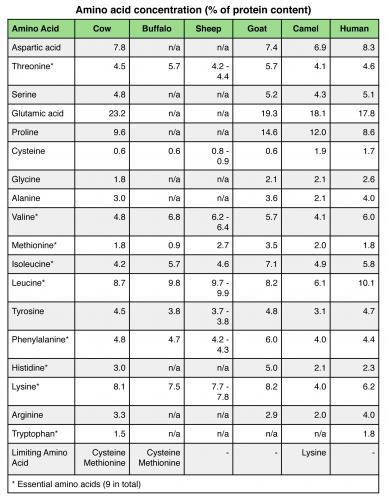
The first group, the essential amino acids, cannot be produced in the body, so must be consumed in the diet.
How much protein?
We’ve learned that the nucleotide sequence in our DNA determines the sequence of amino acids in polypeptides. We also know that the shape or additional groups attached to proteins control their function, so affecting the phenotype, or observable characteristics, of an individual.
Most proteins, despite being the second largest constituent of our bodies after water, are in a constant state of turnover. While some may exist for months or even years in the body, many will be turned over in a matter of days. Protein turnover also changes according to age, life stage, level of activity, health status and adaptation to particular levels of protein intake. A person on a lower level of protein intake will tend to recycle amino acids more efficiently and will excrete less nitrogen via the urine (and to a lesser extent the faeces) so that nitrogen balance achieves—within a given range of intakes—a steady state based on input and output.
Do we then just have to make sure that we’re getting the bare minimum of essential amino acids from our diets, and at particular times in our lives (e.g. during rapid growth, pregnancy, lactation, illness) make sure the conditionally essential ones are also provided, because our bodies will find, or adapt to, a steady state?
In essence, this was the basic approach for many years and dictated how the minimum protein requirement in humans was determined. These determinations have largely been made on minimal levels required to achieve nitrogen balance and on the most limiting amino acid, for example, essential branched-chain amino acids, especially leucine, which are key to the regulation of muscle protein synthesis. This approach has spawned the protein digestibility-corrected amino acid score (PDCAAS) approach, introduced by the Food and Agriculture Organization of the World Health Organization (FAO/WHO) in 1991. The PDCAAS is the current internationally approved method for protein quality assessment. However, given the complexities of metabolism and protein utilisation in different individuals, the use of laboratory and theoretical models on which to draw and compare data, even the FAO/WHO have concerns about the PDCAAS approach which relies on three key parameters: protein digestibility (measured in a faecal assay in rats), biological value and amino acid score. The PDCAAS approach has thus been subject to academic criticism, uses the requirements of a pre-school age child to determine limiting amino acids, takes no accounts of where in the gut proteins are absorbed; ignores conditionally-essential amino acids or the role of anti-nutritional factors such as lectins in leguminous protein sources consumed concomitantly, and; also ignores if, when and how the ingested amino acids may be utilised by the gut microbia or how other foods affect digestion, absorption or requirement.
It is worth noting also that intake studies have generally involved limited population groups, particularly malnourished ones in developing countries. Findings from these populations are not necessarily transferable to the vastly different lifestyles of Western populations that typically consume a very different amount and balance of macro- and micro-nutrients, as well as having different physiological needs and health status. Body size is another factor to consider, and you may find it interesting to use The Telegraph newspaper’s calculator to compare your body weight with average body weights around the world!
In the UK, the Reference Intake for protein has been set at 0.75g per kg body weight. In the USA, the Dietary Reference Intake for protein has been set, unsurprisingly, a fraction higher at 0.8g per kg body weight. That equates to around 52 - 56 g for a 70 kg adult depending on if you use the UK or US reference amount.
The Spanish study we rebutted last week points towards these levels as determined by the PDCAAS method being about right.
However, there is an emerging body of evidence showing that high quality proteins in amounts greater than the reference amounts dictated by governments (using the questionable PDCAAS approach) have a range of other benefits, that extend well beyond simply the maintenance of muscle mass, bones and essential metabolism.
This may include body weight and fat mass loss, maintenance of lean mass (including avoiding or reducing age-related muscle loss or sarcopenia), and reduced risk of neurodegenerative conditions, such as Alzheimer’s disease.
A major review of all the available evidence just published in the American Journal of Clinical Nutrition, looking at available studies and meta-analyses (studies of studies) has just been released and confirms, overall, that protein intakes significantly above the 0.8 g/kg body weight (bw) level prescribed by the US National Institutes of Health (NIH) better supports healthy weight and muscle management than the prescribed amount.
The ‘sweet spot’ of intake of high quality protein appears to be somewhere between 1 and 1.4 g/kg bw for most adults, dependent on gender, life stage, physical activity, health status and other factors. Mean intakes of protein in the US, as in the UK, are presently about 88 g/day, equating to around 1g/kg. But an increase in protein of around 25-30 g per day, compared with this average level, was found to give rise to significant improvements in healthy weight management and bone health.
Tampering with nature’s proteins: Processing and cooking
It’s the processing and cooking of proteins that is likely the root cause of the risks that have sometimes been related to high protein diets, including the recent Spanish study.
High temperature cooking, oxidation and other treatments are applied to many protein-containing foods, especially meats. Their purported benefits are increased shelf-life, reduced risk of food-borne disease and aesthetics. But they can lead to the formation of compounds which interfere with protein uptake in the body and within cells. These include Maillard compounds (heat-related browning), oxidised sulphur amino acid, D-amino acids, or cross-linked peptide chains, which limit amino acid bioavailability. Additionally, the carbonisation of meats, including proteins and fats, can lead to the formation of carcinogens such as PAHs and HCAs.
Glutamate and cancer
Another argument sometimes put forward about higher protein intakes has been linked to the risk of over-supply of glutamate, which in turn can be used in place of glucose to feed tumours in the body.
Glutamine science is something of a conundrum; while glutamate can feed cancer cells, low glutamine adversely impacts the amount of glutathione, which in turn affects natural killer cells and nitrogen balance that protect against cancer. Research suggests that cancer cells are so glutamine-dependent that they can probably source all the glutamine they need to proliferate even with low levels of protein intake. But in such cases of low intake, or if you choose to consume proteins with an amino acid profile that minimises glutamine, it appears likely that your cancer protective machinery will not have sufficient resources to function properly.
Supporting this view is the growing body of clinical research which shows that glutamine supplementation can be cancer protective - probably because it feeds our body's cancer-fighting machinery.
Protein supplements for the elderly
Older people need more protein to offset issues with bioavailability that appear not just to be related to reduced digestive potential. Dr Andrew Murton from the University of Nottingham makes a strong argument for older people consuming high digestibility protein supplements (say 25-40 g/day), to be used alongside resistance exercise training. This not only helps to stave off sarcopenia but also helps to maintain skeletal strength. It’s something of a disgrace that such recommendations have not found themselves into government or health authority guidelines – but the general anti-supplement stance of governments is legendary and seems to be upheld irrespective of the state of the science.
Food quality, the presence of friendly bacteria in fermented foods and probiotic supplements and prebiotic fibre are also critical to help maintain a healthy gut microbiome. The microbiome can play a central role not only in protein and other nutrient absorption in the gut, but also as a modulator of the immune system and of brain function.
Important for many, is avoidance of lactose, a naturally-occurring and therefore unlabelled ingredient in whey concentrate and casein protein supplements, and fillers, such as maltodextrin, that provides an often unwanted source of refined carbohydrate (see below). Avoiding protein supplements that include artificial colours, flavours and sweeteners is also advisable.
Protein and carbohydrate combining with exercise
A final point on ‘when’, especially in relation to exercise.
While there is a commonly held view among sports scientists that carbohydrate should be consumed alongside protein (e.g. in 2 or 3 to 1 ratio) in the one hour window after training to promote protein synthesis and protect against protein loss in muscle tissue, trials underpinning this view are both very limited, conflicting or involve misinterpretation of results from existing trials.
Without nutritional support, any form of more intense or longer duration exercise will cause a negative muscle protein balance. Critical to both muscle protein building and protection against muscle breakdown is the availability of amino acids and insulin. The latter is always present in the circulation even in a fasted state, but is triggered to some extent by protein ingestion and to an even greater extent by carbohydrates.
It has been known for over two decades that consuming protein with a plentiful supply of a diverse array of amino acids, especially leucine, is critical to increasing synthesis, while raised insulin, alongside AA availability, is important to protect against muscle protein breakdown.
While insulin is required in conjunction with leucine and other amino acids to promote synthesis, there is good evidence that the low levels in circulation, even in a fasted state, are sufficient. Raising these by up 30 times over the fasted level has not been found to further induce protein synthesis.
As far as protecting against protein degradation in muscle following exercise, there is also good quality evidence from human trials showing that the small spike in insulin that is triggered by consuming protein alone is sufficient to protect against protein degradation in muscle. This has been confirmed in an important trial that showed no further protection against protein loss was achieved when carbohydrate was consumed alongside protein, as compared with protein alone.
Further reading:
Re-thinking your food choices for 2015
The starting point for metabolic flexibility



Comments
your voice counts
21 May 2015 at 3:13 am
The main reason people don't eat enough protein is that they are terrified of eating any animal fat, expecting their arteries to instantly clog-up. This fear is caused by Mainstream Med's misinfo.. that to market the 'bad cholesterol' lowerng, totally useless and highly toxic statin drugs. They can't tell you animal fats protect arteries, and don't fatten, and then tell you to 'lower bad cholesterol' with statins.
26 May 2015 at 9:06 am
Protein is a vital nutrients that your body needs to function properly. Everyone needs protein on regular basis but athletes needs more because they burn more calories. Often it seems to be difficult to eat enough protein containing foods on a regular basis to get the enough amounts needed. This is where protein supplements are important.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences