
Content Sections
By Rob Verkerk PhD
Founder, executive & scientific director, ANH-Intl
Kids and parents who don’t follow national guidelines for vaccination are becoming increasingly stigmatised. Parents on both sides of the vaccination divide believe they’re doing the best for their kids. In California, some vaccinations are required for a child to attend school while in Australia the ‘No jab, No pay’ rule means parents don’t get benefits if their kids are not fully vaccinated.
Governments claim vaccines to be both ‘safe’ and ‘effective’, despite often weak, misrepresented, manipulated or non-existent evidence. The US National Vaccine Injury Compensation payout of US$3.5 billion to vaccine damaged children over the 28 years since the program was established is evidence that vaccines can do considerable harm.
Any proper recognition by governments of a link between vaccines and injury opens governments, and consequently vaccine manufacturers, to liability. Vaccine manufacturers hide behind government guidelines, protecting them from liability. This is clearly shown in the US Centers for Disease Control cover-up exposed in the documentary Vaxxed shown last night in London.
Wakefield witch-hunt
Obscuring any evidence of a link is the primary driver for such vigorous challenges against those in authoritative positions who suggest vaccines may be risky. The UK General Medical Council (GMC) finding of professional misconduct against Dr Andrew Wakefield after he and his 12 co-authors highlighted the possible association between the MMR vaccine and gastro-intestinal diseases remains one of the most prominent cases.
Much less well publicised is that the senior author on Wakefield’s subsequently retracted 1998 Lancet paper, Prof John Walker-Smith, who also had his medical license revoked after the GMC hearing, was completely exonerated of all charges in 2012 following his High Court appeal.
Misinformed choice
Lack of informed choice happens because of a huge imbalance in the information made available to consenting parents around the time that vaccinations are offered. By looking at a small part of this huge and complicated area, notably infection by the measles virus and the MMR vaccine, we provide below an example of how parents are pushed down the vaccination route, without being given adequate alternative options to help them best protect their children.
All countries within the European Union offer vaccinations to children against measles, mumps and rubella in the second year of a child’s life.
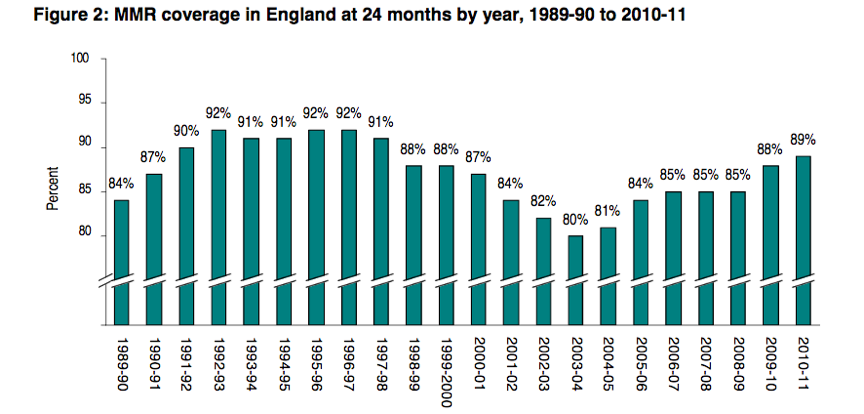
In the UK, vaccination rates for MMR have been high (ca. 90%) since the introduction of the triple MMR vaccine in 1988 (see figure below). This timing coincides with the time that autism rates rose dramatically, and a huge effort has been expended to quash any suggestion of a causal link. The main reason there is such an international, government and pro-pharma effort to shut down showings of Vaxxed is precisely because the documentary shows that in the most important study to test for a link between autism and the MMR vaccine, the CDC manipulated data.
However, there was a distinct hiccup in the mid-2000s owing to concerns about MMR’s safety linked to publicity around Wakefield et al’s Lancet paper suggesting a possible link between MMR vaccination and bowel disease associated with autism.
In the UK, parents looking for evidence of effectiveness of the MMR vaccine, or those who ask this question of their doctors, are invariably drawn to the key figure that can be found on Paediatric Care Online (or one similar), excerpted below.
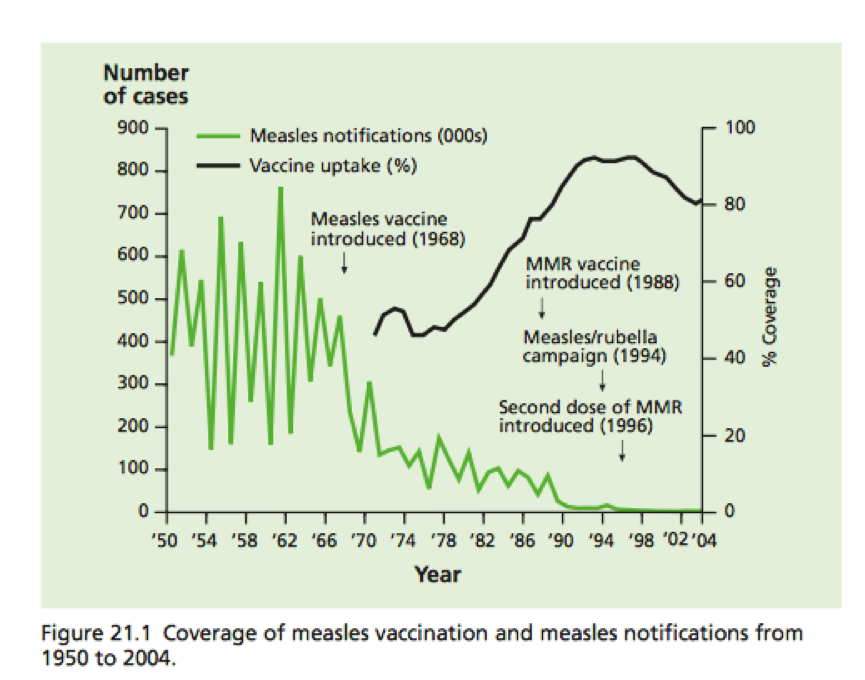
This figure appears to show measles rates oscillating, somewhat steadily around 500,000 cases per annum prior to 1968, when the measles vaccine was introduced. Then suddenly, apparently when the single vaccine was introduced, measles infection rates started to plummet and they were reduced further when the MMR vaccine was introduced in 1988. Then when the second MMR dose was introduced in 1996, as if delivering the final blow, measles infection was almost completely eradicated in England and Wales.
It’s a persuasive story. But we think it’s misleading to associate the vaccines so completely with the decline in measles infection rates. If you look at long-term trends, say going back to the start of the 20th century, measles (infection and associated mortality) was already in steep decline.
This is shown clearly by UK government data, as presented in the figure below.
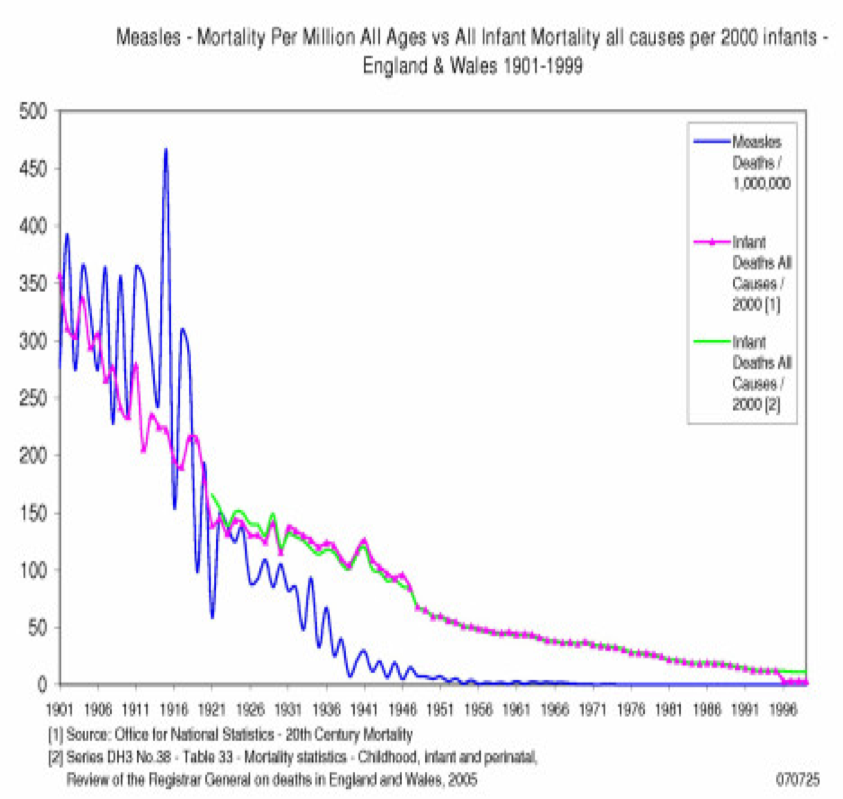
This data shows why the vaccine expert, Professor George Dick wrote in the British Medical Journal (BMJ) in 1980, “measles appeared to be becoming a trivial disease in a civil society. There is something to be said for allowing a mild “wild” measles virus to give natural life-long protection to a community and to offer vaccine selectively to those who are most vulnerable or who have escaped natural infection in the early years of childhood.”
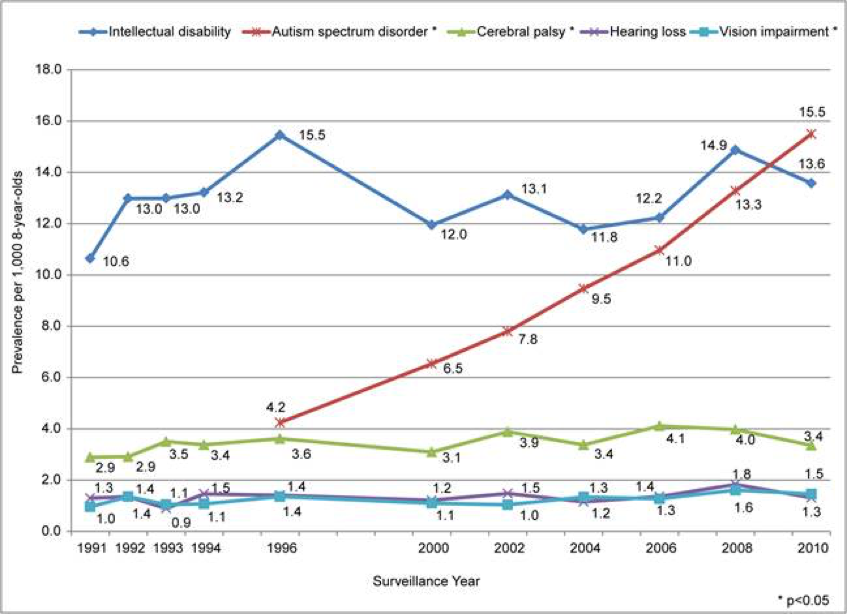
And we shouldn’t of course ignore the all-important rise in autism, as shown in the following figure from the Age of Autism, that suggests that the rise cannot just be associated with improved diagnosis given the comparison with other conditions.
Informed choice
At ANH-Intl, we have long campaigned for informed vaccine choice. We are not anti-vaccine per se, but we believe those who choose to vaccinate should be given the necessary information to equip them with making decisions that are in the best interest of their children’s health.
Given the rapidly accumulating data on the effects of vaccines, antibiotics, birthing method as well as dietary and lifestyle patterns on immunity, it is perverse, in our view, that more comprehensive and relevant information is not given to parents who have concerns over the safety of vaccines.
While in most parts of the world, including in Europe, parents may choose to vaccinate or not vaccinate their children, no government or health authority yet provides information on enhancing a child’s immunity in the event that they should choose not to vaccinate.
More and more science points to the fact that children who are more exposed to microorganisms at a young age are less likely to mount an effective immune response following vaccination (i.e. ‘hygiene/microbiota hypothesis’), making vaccination less effective than in children who have been less exposed (e.g. born by caesarean section, those on repeat antibiotic prescriptions, or those who spend time predominantly indoors).
Additionally, health authorities, owing to their intimate tie-in with the vaccine and pharmaceutical industry – do not provide alternative strategies for vaccines that reduce the impact on the most precious and sensitive members of our society.
Below, you will find some recommendations, with links to some of the relevant science, for those who might choose not to vaccinate, or who wish to engage with a lighter or delayed vaccination schedule for their children.
Making informed choices on vaccination: Natural immunity and judicious vaccination strategies
- ANH-Intl Food4Health guidelines
- Rutayisire E, et al. The mode of delivery affects the diversity and colonization pattern of the gut microbiota during the first year of infants' life: a systematic review. BMC Gastroenterol. 2016; 16(1): 86.
- Bezirtzoglou E, Tsiotsias A, Welling GW. Microbiota profile in feces of breast- and formula-fed newborns by using fluorescence in situ hybridization (FISH). Anaerobe. 2011; 17(6): 478-82.
- Yang I et al. The Infant Microbiome: Implications for Infant Health and Neurocognitive Development. Nurs Res. 2016; 65(1): 76-88.
- Li M, Wang M, Donovan SM. Early development of the gut microbiome and immune-mediated childhood disorders. Semin Reprod Med. 2014; 32(1): 74-86.
- Turta O, Rautava S. Antibiotics, obesity and the link to microbes - what are we doing to our children? BMC Med. 2016; 14: 57.
- Logan AC, Jacka FN, Prescott SL. Immune-Microbiota Interactions: Dysbiosis as a Global Health Issue. Curr Allergy Asthma Rep. 2016; 16(2): 13.
- Robert W Sears, MD. The Vaccine Book: Making the Right Decision for Your Child (2011, Sears Parenting Library). Dr Sears also recommends avoiding any vaccinations for diseases that have already been contracted by a child given that immunity will have already been naturally established.



Comments
your voice counts
15 February 2017 at 10:40 pm
Good, keep these articles coming! I have just had an email from one of my patients (mother of an autistic child) who told me that when she posted the ingredients of the MenC vaccine (which she downloaded from the CDC!) on a parents' network the admin took it down because "it is anti-vaccination and we don't want that here".
16 February 2017 at 9:10 am
Thanks for sharing Uschi. It's a sad world we live in where people are too held in the grip of fear to open their minds to new information. If for no other reason than because science is ever moving and our knowledge is continually evolving. With that evolved knowledge comes greater understanding of how our actions may be causing unwanted impacts - be they health or environmental. If that weren't the case in medicine we'd still be in the dark ages! The whole issue round vaccines is so emotionally loaded though because it's completely contra to our DNA for parents to consider that they may have unwittingly engaged in actions that have impacted their children's health. It's better to shut it out and not know. As Andrew Wakefield shared with us at our meeting on Tuesday evening, many parents, doctors, scientists and regulators alike are choosing to live in what he calls "<em>cognitive dissonance</em>" because it's more comfortable. The tide is beginning to turn though. Vaxxed is really not an anti-vaccine film. It's about understanding how scientific fraud at the highest level has knowingly put children in danger and is responsible for damaging children. These are facts everyone should know about in order to make informed choices. Best, Meleni
17 February 2017 at 4:26 am
I am writing to you whilst staying in Australia and am so concerned at the propaganda which is promoted on TV. A GP casually states that immunisation has been shown to be safe for young children. This along with the 'no jab, no play' message and I think witholding of child allowance it is, is threatening and coercive behaviour. Where is the non biased research and information so one can make an INformed decision.
17 February 2017 at 7:26 pm
Hi Jo, thanks for sharing. It's easy to get despondent about what appears to be the dumbed-down, controlled and undemocratic reality when it comes to vaccine choice, but we are reaching a tipping point through the sheer numbers of people around the world who feel the way that we all do. There have been various attempts to pull relevant data that provides the basis for more informed choice together in book form - one such book is by Suzanne Humphries MD - http://anhinternational.org/2013/10/02/anh-book-review-dissolving-illusions-by-suzanne-humphries-md-and-roman-bystrianyk/. You can find additional information on her website www.drsuzanne.net. Please also find more information on our Vaccine Choice campaign pages. We are in contact with some of the doctors in Australia who are standing up against challenges by state medical boards to their provision of exemptions for children who are either suspected of being highly sensitive or where there is a history of such sensitivity among siblings. It's so important that we all stand together at this time. Best, Meleni
30 August 2017 at 6:39 pm
I wonder why 'measles epidemics' always seem to turn up at the most convenient moments in time :-) And why are there so many more deathly victims now, compared to before the measles vaccine was introduced back in 1963. From the CDC website ( https://www.cdc.gov/measles/about/history.html ): "In the decade before 1963 when a vaccine became available, nearly all children got measles by the time they were 15 years of age. It is estimated 3 to 4 million people in the United States were infected each year. Also each year an estimated 400 to 500 people died..." Of course the CDC is presenting/twisting numbers in a way that makes vaccinations look like the holy grail, but even if one goes along with this (say 500 deaths in 3 million measles cases) this would still 'only' mean a death rate of 0.013% I know, even one person dying of measles is one too many, but in light of the very low death rate of measles, shouldn't it be my (and other people/parent's) decision to 'risk' getting natural immunity for the measles or not? So tired of getting more and more manipulated (and now/soon being forced into this vaccination hype/idiocy). Just a thought...
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences