

Content Sections
By Rob Verkerk PhD
Founder, executive and scientific director, ANH-Intl and scientific director ANH-USA
Last week at the second Lifestyle Medicine Australasia annual conference, this year in Manly, Sydney (Australia), I was given the opportunity to lay bare key elements of a strategy we believe has the potential to transform mainstream healthcare. Many of us around the world are dealing with different pieces of the same puzzle, motivated by our recognition that the existing system is being driven by various corporate interests at lightning pace into a dead end – one in which innocent citizens will be the main casualties.
There is a long list of factors contributing to the inevitable catastrophe if a business as usual approach continues. Following is our top 10 list:
10 reasons why the existing health and care system is set to fail
- Rapid escalation of the incidence and burden from non-communicable diseases, chronic, “largely preventable” diseases, like cancer, heart disease, type 2 diabetes and obesity
- Increasingly sedentary behaviour and lack of physical activity
- The low rate of success by the healthcare and public health systems in either treating or preventing these diseases
- An increasingly top-heavy age structure with accompanying disease burden
- The rise of antibiotic resistance and consequent resurgence of infectious diseases
- The incapacity of our health, social and care systems to handle the mental health and dementia burden
- Disparities in access to, and effective public health information about, dietary and lifestyle mediated disease prevention and management
- Disproportionate research emphasis, medical education and health authority prioritisation of pharmaceutical-based interventions many of which have limited or unknown effectiveness, especially in relation to chronic diseases and mental health conditions
- Increasing simplification of our diets and loss of nutrient density in plant foods
- An ever-increasing environmental toxin burden in which children are particularly vulnerable.
This multi-faceted, multi-layered problem is inexorably linked with industrialisation, globalisation and the rise of corporatocracy, in which, presently, just 147 corporations control 40% of global trade.
Many organisations are looking at possible solutions. In particular, scientists, sociologists and other academics in universities and other research institutions are being tasked to hunt down possible solutions. But when most of their funding originates from the very corporations that are contributing to the problem, can we really expect independent analysis and conclusions?
We are of the view that independent non-profits like ANH are unusually well placed to consider the options that might be necessary to reframe how we deliver and receive healthcare.
As presented at the conference this last weekend, following are the 8 elements I proposed that need to be changed before we are ready to usher in a system of healthcare that is truly sustainable. Many people have argued that we need to do more work on looking for solutions to chronic diseases like type 2 diabetes, obesity and heart disease, amongst the biggest killers in society. Our view is we already have sufficient knowledge to deal with these issues. However, we don’t have the political will to make the changes we need because the system we rely on for our health and social care is tied so closely to the healthcare services and drugs that for nearly half a century we’ve hoped would yield a solution.
We can no longer wait as catastrophe awaits us around the corner. More than this, treating the tail end of the problem does nothing to deal with the underlying causes of the problem that are rooted in our inappropriate behaviours, diets and lifestyles.
We therefore need to reframe our entire system and to do this, we’re suggesting there are 8 areas at least in which concerted effort is urgently needed. I describe each below in brief.
ANH-Intl’s 8-point Sustainable Healthcare Action Plan
- Re-evaluate ‘the health and social care system' - Typically we think of the healthcare system as being composed of healthcare providers like doctors and nurses, in primary (e.g. general practitioners, nurse practitioners) and secondary (e.g. specialist) care. But actually, we need to think about our health and social care providers in a much wider context. Because healthcare encompasses those measures guided, supplied by or administered by third parties, it has to include food suppliers, fitness and sports specialists, masseurs, integrative medicine and CAM (complementary & alternative medicine) practitioners. The social care system doesn’t just involve institutional care, but also familial care. On this point, it was enlightening to hear Ann Weldon who opened the conference, gave the welcome and introduction on behalf of the Aboriginal people of Australia, say that the word disabled does not exist in her Wiradjuri language. She said if someone is blind, we (those who can see), act as the eyes. If someone can’t walk, he or she will be carried. The Western model of community care is a far cry from the model that has existed so long among indigenous people.
- Re-evaluate what we mean by ‘health’ and ‘care’ - Health is so much more than simply the absence of disease. There is growing consensus that the concept of resilience, which is essentially the ability of an individual to tolerate and recover from any kind of stress be it physical, physiological or emotional, is key. Also, when we think of ‘care’, this shouldn’t just include care coming from a healthcare provider. It should include support from society, from family and friends and, probably most importantly, self-care.
- Re-evaluate the concept of ‘patient’ - While we might think of the patient as someone who receives any kind of healthcare service, the word ‘patient’ is typically interpreted as referring to a "suffering or sick person under medical treatment". The word is derived from the Latin word ‘patiens’ that literally means ‘one who suffers’. The difficulty is that acceptance and general use of this term for any person who receives any kind of healthcare service lulls the public, as well as healthcare providers, into thinking services should be targeted primarily at those who are already ill or diseased. This approach is not consistent with what is required for a sustainable healthcare system, in which most emphasis needs to be placed on healthy people and efforts that keep that majority healthy and free from disease.
- Re-evaluate the lens through which we view human/environmental interactions - It is becoming ever clearer that the most appropriate lens by which to view human health is an ecological one, given the complex interactions which occur within the internal environment of a human with his/her microbiome, and between the internal and external environment. This is a far cry from the reductionist approach that is presently most commonly used.
- Re-evaluate multi-layered system of disease causation and perpetuation - Modern medicine is still wedded to a largely linear concept of cause and effect when it comes to looking at the origin of diseases. This approach has led to major errors of understanding, such as the cholesterol hypothesis (myth) of heart disease. Chronic diseases are actually multi-factorial and multi-layered, and this complexity has been well demonstrated for type 2 diabetes (Fig.1).
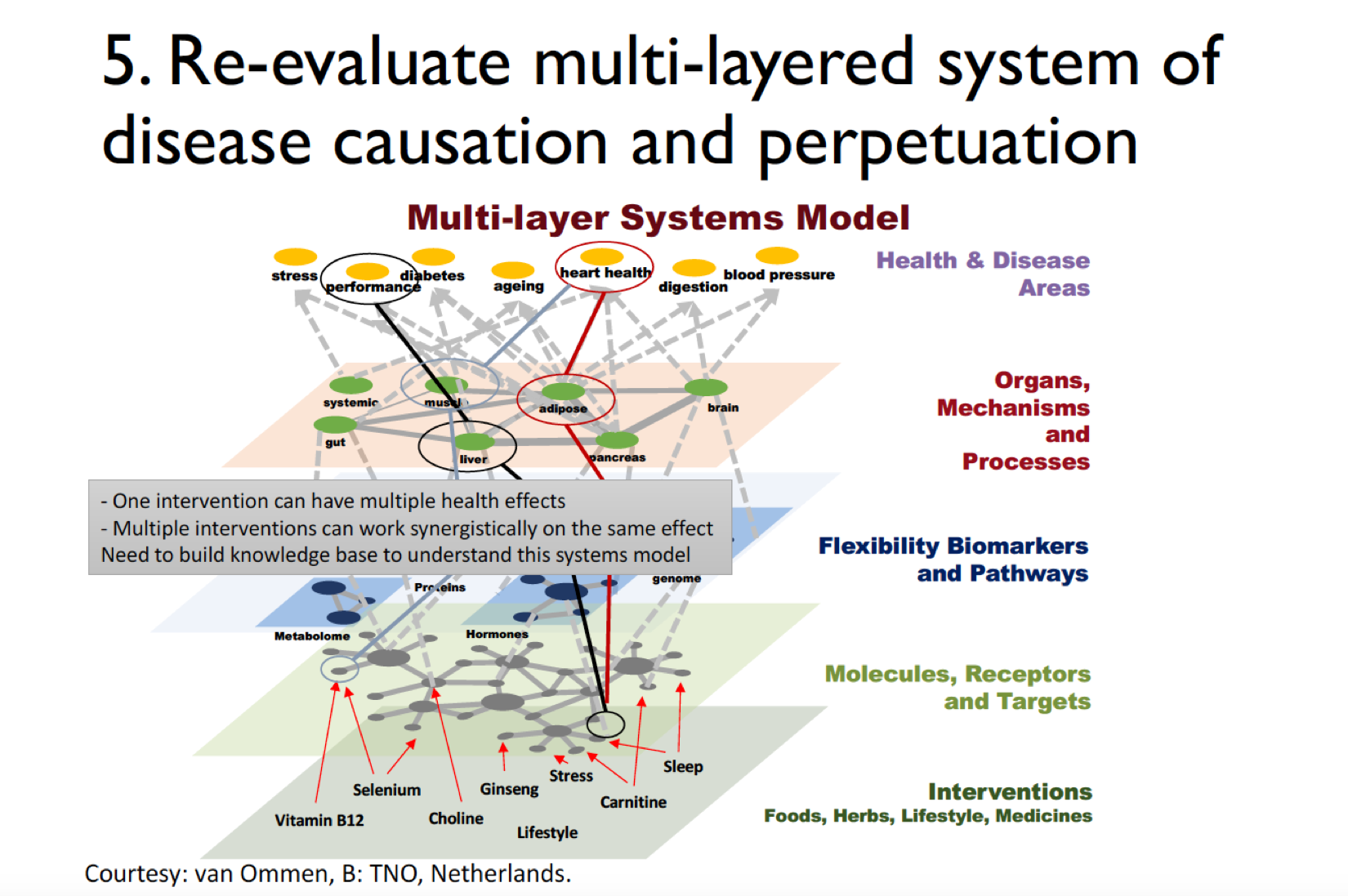
Fig 1. Multi-layer systems mode for type 2 diabetes (courtesy van Ommen, B, TNO, The Netherlands).
We need to consider that so far at least 135 different metabolic pathways have been elucidated in humans, involving 7439 reactions and 2626 metabolites. These work as part of a highly complex network that is strongly influenced by our epigenetic background.
- Re-evaluate the scientific methods we use to select ‘effectiveness’ and healthcare decision-making - The randomised controlled trial (RCT) that has been developed particularly to test drug efficacy and the widely used evidence-based medicine (EBM) hierarchy are both wholly inappropriate for evaluating the effectiveness of the behaviours that are most likely to prevent or reduce incidence of chronic diseases. There isn’t general acceptance of any alternative methodology. Even prospective cohort studies, observational, epidemiological and case control studies that sit near the base of the EBM hierarchy can’t adequately take into account the multiple factors that influence health outcomes in different individuals, let alone their relative importance.This dilemma has been an important trigger for our involvement and scientific leadership in the Hawthorne project. The app that is undergoing development with our research partners allows individuals to collect health data that has two main purposes: 1) to motivate the individual to improve his/her health, and 2) to provide big data to help establish associations between an individual’s level of perceived health and specific human behaviours. For more information, check out our poster presentation given at the conference.
- Re-evaluate our priorities and desired outcomes - We need to have a clear understanding of the objective of healthcare efforts. Is it to treat existing diseases, or is it to prevent disease? Or it is to establish the highest level of vitality and resilience among individuals in a manner that is sustainable and accessible to everyone? Our sense is it is all of these things, but we need to place much more emphasis on the last.
- Re-evaluate our society’s respect for human dignity, freedom and democracy - In a world in which corporatocracy increasingly rules, in which governments are removing more and more individual freedoms ostensibly to protect the health of the public at large, it is going to become ever more difficult to develop a sustainable healthcare system. Such a system requires that the individual is empowered to take full responsibility for his or her own health.
Our work internationally, especially in Europe and the USA, is all about protecting our fundamental right and freedom to choose the healthcare of our choice, especially to self-care. We must therefore work collectively to resist efforts by governments and corporations to limit these freedoms.
Download presentation
Download my 35-slide presentation from this year’s conference organised by the Australasian Society of Lifestyle Medicine.



Comments
your voice counts
There are currently no comments on this post.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences