

Content Sections
By Rob Verkerk PhD; founder, scientific and executive director, ANH-Intl
Those of us who run our health largely by natural means are still a small bunch by comparison with those who believe their local GP’s prescription will deliver their best health outcomes. Nearly 1 in 4 Americans over the age of 40 are on statins and the UK is pushing to get all men over 60, all women over 75 and a growing band of high risk over-30s on the drug. If that wasn’t enough, there’s a strong push to put thousands of children under the age of 10 on statins. And it’s not just heart disease that statins supposedly protect against, it’s cancer, multiple sclerosis and more. Such is the promise of statins, it's routinely referred to as the ‘wonder drug’ by media around the world.
Confused science, doctors and patients
Confused by the science? If you’re not, you should be! There’s a mass of research going on looking at benefits other than a reduced risk of heart attack or stroke. Take autoimmune diseases that are an ever-increasing problem. Some research suggests statins can have immune-modulating effects so might be helpful in the treatment of autoimmune diseases. In direct contrast, there are now at least 28 statin-induced autoimmune diseases that have been identified. One such disease is Statin-Associated Autoimmune Myopathy. As for statins, there’s good work showing that there’s more evidence that statins promote rather than protect against cancer.
Superimposed over these mixed messages from science and from health professionals is of course personal experience or the experiences of friends and relatives. As many as 20% or more of people taking statins suffer a plethora of side effects, from muscle pain, muscle weakness, headaches and dizziness to liver damage, cognitive impairment, nose bleeds, digestive problems, contrast induced nephropathy, cataracts, erectile dysfunction, venous thromboembolism, raised blood sugar, diabetes and, as mentioned above, autoimmune diseases. Depending on what their doctors tell their patients, or on how successfully doctors can convince their patients that the possible lower risk of a heart attack or stroke outweighs the side effects (or ‘intolerance’), people either carry on medicating themselves – or they stop.
Big Pharma manipulation
The media, for which many people are still dependent on for health information, is another major influence in shaping the public’s opinions and it’s no surprise that the pharmaceutical industry has a massive influence on headlines and other content. As Big Pharma’s impact is so pervasive, it’s also unsurprising there have been many calls to curb its influence.
Take, the UK’s Telegraph newspaper as an example. It could be argued that on one hand this ‘broadsheet’ strives to take a balanced view of controversial issues and, on the other, it is widely read by more affluent socio-economic groups who are in turn more likely to opt for non-drug-based approaches to cardiometabolic disease prevention. Following is a grab from a search on ‘statins’ carried out earlier today (Fig 1).
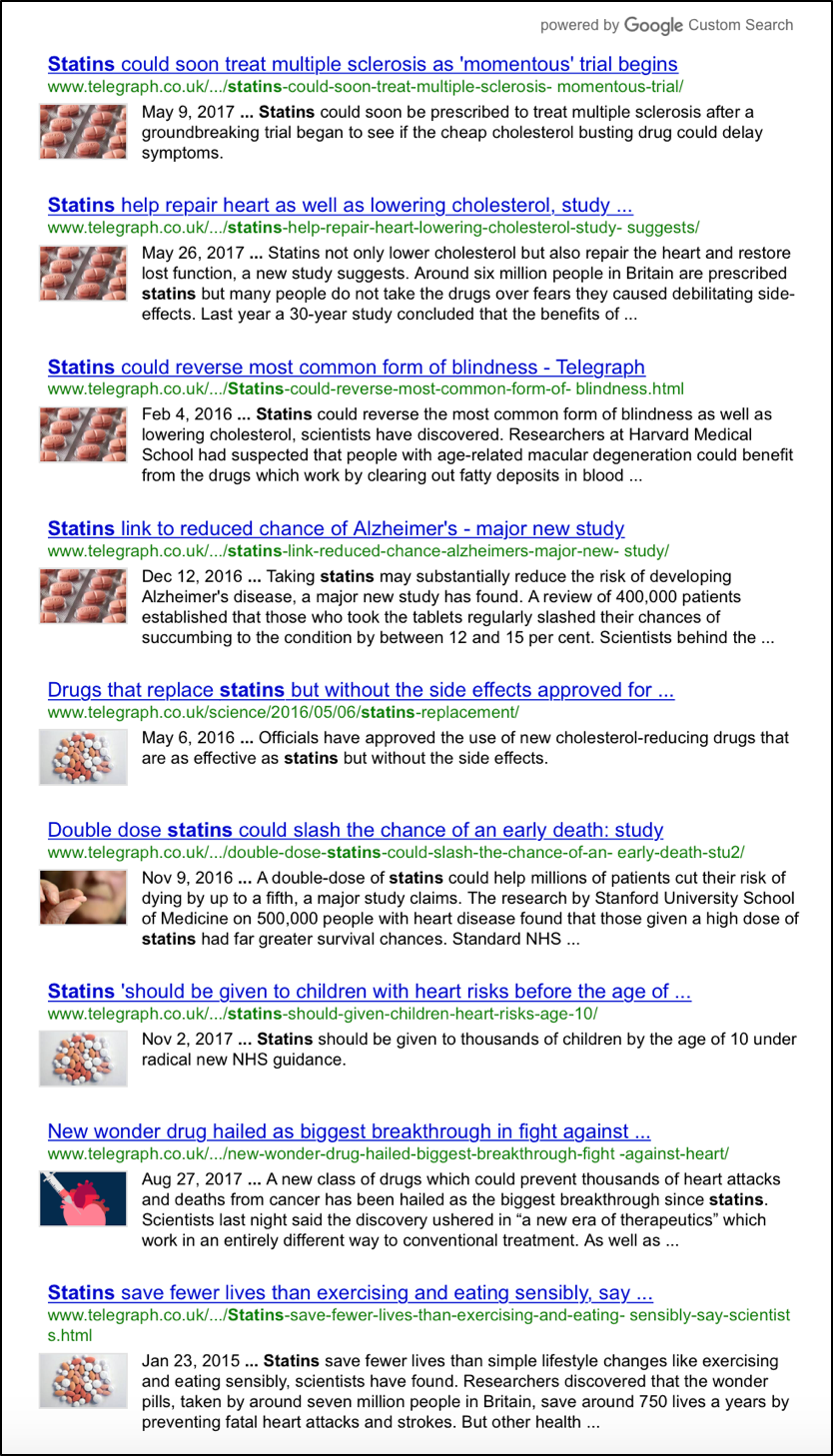
Fig 1. Partial results of online statin search on The Telegraph newspaper website, 7 February 2018
The evidence: diet and lifestyle outperform statins
This is just the first of 10 pages of results. What’s more, you’d have to get to the ninth item – at the very bottom of this grab – to find a single piece of content that reveals something that will ‘speak’ to those more inclined towards a non-drug approach to heart disease risk reduction. The paper the article links to is a study published in 2015 in BMJ Open led by University of Liverpool epidemiologist, Prof Martin O’Flaherty.
Critically, the study finds that population wide measures involving improved diets and exercise deliver far greater benefits than statin therapy targeting high risk groups in terms of heart attack or stroke deaths prevented or postponed. But the models also reveal a perennial issue in research on dietary and lifestyle modifications versus drugs: those in higher socio-economic groups tend to benefit more than those in lower ones. For drug companies, especially in the UK, where approved drugs are dispensed freely or are subsidised by tax-payers, this is something of a nirvana: you get to sell in your product to the National Health Service (NHS) with the ‘feelgood factor’ that you are narrowing the disparity between social classes.
You have to dig deeper still to find a piece in which Dr Aseem Malhotra and others challenge the findings of a Lancet study in The Prescriber, and are quoted as saying: “Decades of misinformation on cholesterol and the gross exaggeration of statin benefits with downplaying of side effects has likely led to the overmedication of millions of people across the world. The lack of transparency in the prescription of statins is just one symptom of a broken system of healthcare where finance based medicine has trumped independent evidence and what is most important for patients.”
Deeper still, you’ll find the view of a British heart surgeon Dr Haroun Gajraj who ditched statins in 2014 after 8 years on them. His change of heart (pun intended) wasn’t because of side effects but rather because his cholesterol was lowered much more effectively by changing his diet and lifestyle than by taking statins.
If you focus on prevention…
Our view at ANH is that the main reason we have over-medicated populations with socio-economic disparities in personal responsibility for health, particularly in terms of prioritising non-drug-based approaches, is because we – as a society – have yet to give prevention enough public and community health focus.
A big obstacle is down to what happens at the primary care or GP level, although it’s interesting that large numbers of GPs already don’t prescribe statins as heavily as the relevant NICE guideline in the UK suggests. That’s important because the GP or family physician, as we’ve already alluded to, still remains in the eyes of many the most important source of information on matters of health.
The multiple barriers to heart disease prevention
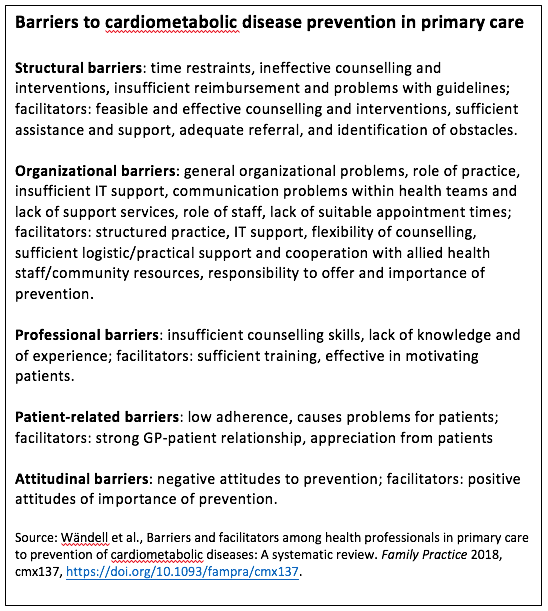
An important paper just published in the journal Family Practice by a group of Swedish and Dutch researchers identifies key barriers to cardiometabolic disease prevention. We believe this provides exactly the right kind of framework that lets different groups in society tackle the multi-faceted issue from multiple vantage points. This is the only way to deal with heart disease and stroke prevention effectively – and that means by not relying on statins.
The authors identify a plethora of barriers to effective prevention in primary care, dividing the barriers into 5 different categories, namely structural, organisational, professional, patient-related and attitudinal:
Take back control
So where do we go from here? Here’s 5 things you can do:
- If you’re on statins already, consider non-drug alternatives involving dietary and lifestyle change as they are likely to work better than statins alone. Consult with a suitably qualified and experienced integrative or other natural medicine practitioner to help you fine tune your program.
- If you continue taking statins, at least supplement with coenzyme Q10, vitamins D3 and K2 that are depleted by statin therapy and contribute to side effects.
- If you’ve experienced statin side effects, make sure you’ve told your doctor and make sure s/he has reported your side effect.
- Engage in a healthy lifestyle that includes not smoking, limiting alcohol, engaging in daily physical activity and consuming a healthy diet based on the Food4Health guidelines. If your heart attack/stroke risk profile has improved because you’ve changed your diet or lifestyle, make sure your doctor knows about it. Remember, the principle contained in the Hippocratic Oath: Primum non nocere - First, do no harm. Hippocrates' advice still holds.
- Share among your friends, relatives and wider contacts those diet and lifestyle modifications you’re making that don’t cost money – or might even save you money. Now more than ever, we need to help dismantle the notion that healthy diets and lifestyles are expensive and only relevant to the more affluent socio-economic groups.
Go to sustainable healthcare campaign



Comments
your voice counts
07 February 2018 at 8:05 pm
snip/
The 'Medical State' is not science, nor the state it still at times pretends to be. It is a facet in a system of mind control, in which we think our thoughts are our own, rather than something that is not truly belonging, given free access to think in our stead.
I essay these sketches in the wondering if it is possible to say this and be received - and whether such a shared moment is a light in a sleeping humanity by which others can stir from a different purpose than salvation by separation from the feared and hated.
I am living my choice, in witness to that we are beings of choice. But fear-defined thinking frames only the choices that keep us fixated in looking away from Cause - because in between us and our original or true nature is a gap that fear made, to protect itself.
Why did I write this? I felt the article above is pussyfooting around the issues - when of course the between the lines message is - we are being manipulated and deceived and need wake up to a true basis from which to discern what is worthy and what is seeking to pass off as if it has worth or means what it purports.
snip/
07 February 2018 at 10:11 pm
Part of the difficulty with disease prevention is the relatively poor benefits from a 'one size fits all' approach.
Individual variation means that different strategies within the overarching principles are often needed to produce optimum results in different people. When the strategies are not optimum, the benefits are reduced, people do not notice increased subjective wellbeing, and compliance is reduced. The skill of self-selecting which lifestyle advice to follow needs to be taught.
Despite so much evidence, there is still a poor understanding in the population and among health professionals, of just how powerful appropriate prevention (diet and lifestyle) can be.
07 February 2018 at 11:18 pm
In item 2 above does the sentence end ("...and contribute to side effects.") mean "...thus contributing to side effects"?
08 February 2018 at 10:19 am
Thanks Rob for your ongoing concern and real activity (clear, precise, researched and eloquent articles) aimed at helping people to make informed decisions about their health and wellbeing! Brilliant!!
08 February 2018 at 5:37 pm
My husband has high cholesterol (8 mmol/l ) together with high LDL. He was referred to Hammersmith hospital for a CT coronary angiogram and carotid artery scan. Both came back 100% clear. No build up in the arteries and he is 60 and has had high cholesterol for ever anyway. I think if his arteries were going to become clogged it probably would have started happening by now. People need to think twice before going on statins for a problem they might not even have.
10 February 2018 at 12:20 pm
Cholesterol is imperative for brain function. Insufficient cholesterol for the brain to operate correctly leads to (the common side effect of Statins): memory loss and the onset of dementia or Alzheimers. Can no one see that the increased prescribing of statins to the population also corrolates with the epidemic of Alzheimers!!!! Big Pharma is a criminal carbal and don't forget about Agenda 21 (which includes depopulation). Check it out!
10 February 2018 at 9:03 pm
I was just discharged from hospital, having had an MI, with a goody bag of pharmaceuticals. Writ large were the statins, notwithstanding the fact that my angiogram showed completely clear arteries, I am a 70 year old woman who has lived on a HF/LC diet for a number of years, and I quote Dr Kendrick: “The statistic you really want to know about statins is the following. If you have had a heart attack, or stroke, and take a statin for five years, you will increase your life expectancy by 4.2 days. Balance that against a twenty per cent chance of having side effects, some of which are very unpleasant and long-lasting, and you can see why I am not a fan of statins.”
Alas, I am not in the good books of the cardiologists nor my GP for refusing statins.
11 February 2018 at 2:32 pm
I have known men who have been put on Statins and when I tell them to go
Back to a different doctor in the practise and ask why....they have been told
They do not have high Cholestrial and there is no reason and have been
taken off. Others who take it experience muscle pain.
My doctor tried to force me to take statins and when I said no.....she
Threaten me with a heart arttack if I did not take.
I am a healthy person with, good diet and exercise.
I stood my ground because I am well informed.....many are not and give in
To the bully attitude
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences