
Content Sections
- ● Diversity rules
- ● What we’re not talking much about
- ● A question of quality and quantity
- ● Units for measuring EMF radiation
- ● So who’s your best friend?
- ● Demystifying frequency devices
- ● Entering the lion’s den
- ● The consequences of poor industry self-regulation aren’t good for natural health
- ● How do frequency-based devices work?
- ● Clean or dirty signals?
- ● Do frequency medicine devices work?
- ● Conclusions
- ● Our appeal
By Rob Verkerk PhD, founder, executive & scientific director, Alliance for Natural Health International
You’ve heard news of a revolutionary frequency-based device that has a list of diseases it can supposedly remedy that would make Pfizer’s R&D team leader quiver. You’ve read dozens of testimonials and your head’s still spinning. Some were from cancer patients who were classified as terminally ill who’ve gone into ‘spontaneous remission’. Others came from people so ill they were permanently bed bound – until their frequency treatment got them walking again. Let’s also not forget the athletes who used it who developed superhuman powers.
Your critical mind tells you this could mean only one of two things. The testimonials are from intensely satisfied people who’d experienced what many might typically classify as a miracle. Or they’ve been fabricated by over-zealous marketeers keen to make a buck.
Any of this sound familiar?
This article is about helping you to make sense of this rapidly expanding sector of primarily electrically-powered frequency medicine devices. We won’t be dealing here with some of the non-technologically dependent modalities of frequency medicine, other than in passing. That includes everything from acupuncture, qigong, reiki and homeopathy, through to hands on healing, crystal therapy, and distance healing. This area of subtle energy medicine – as relevant as it is for many – we’ll leave for another article.
Diversity rules
This is one area where the phrase, “not all [in this case devices] are created equally”, is especially pertinent. It’s also an area where, in the case of some devices, it’s not possible to appraise either safety or benefits because there just aren’t enough technical data available to know what the devices are actually doing as they interact with the human body.
More than this, some devices falling under the amorphous banner of ‘frequency medicine devices’ have actually been found to cause harm. This has been most evident with electromagnetic field based devices used occupationally by physiotherapy operators on a daily basis and for extended periods of time.
Perhaps we shouldn’t be surprised about the potential for harm, given we now know categorically that some low intensity electromagnetic fields that deliver low to mid-range frequencies, such as those used in powerlines, wifi routers and mobile phones, can also do harm, especially to those who are electrohypersensitive.
This article, which follows Part 1 that aimed to show why electromagnetism and resultant frequencies are inexorably linked to life and health, has been written to help demystify the rapidly emerging field of frequency-based devices, as used for assessing aspects of health, or for treating the body, either in healthy people or those with a specific condition.
We also aim to give you the categories of information that we think should be available to anyone who consents to use such a device of this type, in accordance with one of the most important and fundamental principles of medical ethics, namely informed consent. This requires that users of devices are provided with information on the potential risks and benefits of the intervention, before they use it. If a practitioner is involved, properly informed consent also requires that the user is informed of possible alternative interventions so he or she can exercise the freedom to choose.
What we’re not talking much about
There are an incredibly diverse range of commercial devices being used in the health space that rely on frequencies. We won’t be talking, except in passing, about the multitude of electrotherapeutic devices that have been widely used in conventional medicine, especially in physiotherapy, some for over 70 years.
These include a range of technologies that use electrical currents (microcurrents) to trigger nerves and muscles, that induce a thermal (heating) effect often among other effects, such as Transcutaneous Electrical Nerve Stimulation (TENS), Neuromuscular Electrical Stimulation (NMES), Functional Electrical Stimulation (FES), Iontophoresis (which we mentioned in relation to Robert Becker’s work with silver ions and joint healing in Part 1), High Voltage Pulsed Galvanic Stimulation (HVPGS), and the like.
Technologies also used by physiotherapists, that we won’t include here, are thermal methods such as therapeutic ultrasound as that deals with sound waves, which generate acoustic and vibratory frequencies but not electrical, magnetic or electromagnetic fields, as we also discussed in Part 1. Off our list of talking points will also be the use of intense light from lasers, such as Low Level Laser Therapy (LLLT) and High Intensity Laser Therapy (HILT).
So what does that leave us with?
What we’ll be focusing on in the main are the gamut of devices that emit electromagnetic energy that are often also able to measure the body’s own weak electromagnetic fields. These are the kinds of devices that are gaining more and more use in the sphere of integrative or ‘alternative’ medicine and so are the ones most likely to be encountered by proponents of natural health and wellness.
As you may recall from Part 1, any electromagnetic field involves an interaction between both electrical and magnetic fields – and these fields allow the transfer of energy through electromagnetic waves, and that energy can have profound effects on different processes and structures in the human body, from our skin all the way to our DNA.
A question of quality and quantity
If a device professes to be able to read the body’s magnetic field, it needs to be incredibly sensitive given the electromagnetic energy output of the body is extremely weak (which doesn’t make it unimportant) and mediates its effects well below the thermal (heating) threshold.
Thermal (energy) is of course a different matter. We each, as adults, issue around 100 watts of energy, 24/7. This thermal energy, that’s responsible for maintaining our body temperature despite the continuous loss to the environment around us, is generated primarily by all the biochemical reactions associated with our metabolism that in turn release energy in the form of heat.
But it isn’t this thermal energy that ultimately controls the interactions of individual molecules, atoms and sub-atomic particles in the extraordinarily sophisticated way that we know as ‘life’. That’s down to the much weaker and more coherent electromagnetic energy that we considered in Part 1, energy that helps create the crystalline energy of our biofield that in turn provides the matrix for the body-mind being that we think of as the human species.
This electromagnetic energy is always issued in a wave form and doesn’t need a medium (like air or water) to propagate, which is why electromagnetic waves can travel through space. This enables us to see stars with the naked eye, including stars in the Andromeda galaxy that are estimated to be some 2.5 million light years way. Remind yourself that when you look at those stars, the light and image you’re looking at represented events that took place 2.5 million years ago, before the first members of our genus Homo appeared on Earth!
These waves, that are the product of combined electrical and magnetic fields, have 5 key, interrelated properties:
- Frequency – the number of wave crests passing a given point per second, with 1 Hz being equal to one wave cycle per second
- Wavelength – the distance between each wave crest (Fig. 1), measured typically in metres, millimetres or nanometres
- Amplitude (height) of the wave (Fig. 1), that is a determinant of its power or intensity, that is often measured in milliGauss (mG) or Tesla units
- Waveform – the shape of the wave, including whether it’s a smooth sine wave with rounded crests and troughs, or a stepped digital wave, as well as whether the form is continuous or pulsed, or changes in form over time
- Energy – the amount of energy carried by the wave that is dependent on its frequency and in particular its amplitude (wave height; Fig. 1). As Einstein’s general theory of relativity formula E = mc2 reminds us, it is the energy carried through electromagnetic waves that can be converted to matter, and, equally, matter can be interconverted back to energy. Units of measurement of energy vary depending on the type of field being measured. They include milliGauss (mG), nanoTesla (nT), Ampere per meter (A/m), microWatts per square meter (µW/m²), Volts per metre (V/m), or as the Specific absorption rate (SAR), namely the power absorbed per mass of human tissue, expressed as watts per kilogram (W/kg).

Figure 1. The wavelength and amplitude of an electromagnetic wave (sine wave form). Source: European Commission.
Electromagnetic waves – in a vacuum – always move at the speed of light (just under 300 million metres per second). Why? In simple terms, because that’s the speed of light and light is a form of electromagnetic energy as you’ll see from any diagram of the electromagnetic spectrum (see ‘Visible spectrum’, Fig. 2)

Figure 2. The electromagnetic spectrum, showing wavelengths (in metres, including the size of objects that approximate to them) as well as frequencies (in Hz).
Three key parameters of an electromagnetic wave, namely the frequency (Figs. 2 and 3), wavelength (Fig. 1) and energy, are interrelated mathematically – as the great Scottish scientist James Clerk Maxwell proposed in the 1860s and 1870s. So if you know one of the parameters you can calculate the other two, using what are referred to as Maxwell’s or the Maxwell-Heaviside equations.
While you could describe all electromagnetic energy or waves using all three of these parameters, a convention has evolved in physics that means radio and microwaves are commonly described in terms of their frequency (Hz), infrared and visible light in terms of their wavelength (metres [m] or nanometres [nm]) and x-rays and gamma rays in terms of their energy (electron volts, eV). Both x-rays and gamma rays are forms of ionising radiation, meaning they carry so much energy, they can remove electrons from atoms thereby ionising them. An electron volt is the amount of kinetic energy that’s needed to move one electron through one volt potential.
The interrelationship between these three parameters always means that the shorter the wavelength, the greater the frequency, and the greater the energy. That’s why radio waves are widely considered safe, and x-rays and, to an even greater degree, radioactive gamma rays, are so dangerous.
Oh, if only that was all we needed to know about physics to understand frequency-based devices! There are actually a multitude of other parameters that change the biological effects of electromagnetic radiation, these being specific not only to the radiation source but also to the condition and state of the receiving cells, tissues, organs and organism. There is still a huge amount that remains to be explained. But what we do know is that another key parameter is the waveform, which takes into account its pattern, whether it’s continuous or pulsed, and even whether it’s analogue or digital, the former typically being smooth and sine wave like, the latter typically stepped and jagged (unless converted to an analogue signal through a specific piece of technology called an digital to analogue converter or DAC). Electromagnetic waves can also be refracted (bent) in specific directions when they enter particular media – and the amount and direction of refraction is dependent on both the wave type and the medium exposed.
Electromagnetic fields (EMFs) are produced by all forms of electrical or electronic equipment, whether it’s a radio, TV, computer, cell phone, dimmer switch – or an electrically-powered frequency medicine device.

Figure 3. NASA’s classification of the electromagnetic spectrum by frequency, showing both the radio and optical spectrum. Source: NASA
Units for measuring EMF radiation
Despite all these (and other) different characteristics of electromagnetic waves, there are a number of measurements of electromagnetic fields (EMF) that can be readily measured at low cost that give us key information about their potential for biological effects, especially, from what we currently know, their potential to cause harm. These are:
- For the magnetic component of the field, the amount of energy measured in milliGauss (mG) or nanoTesla (nT) (1 mG = 100 nT)
- For the electrical component of the field, the amount of energy measured in Volts per meter (V/m)
- For the radio frequency component, the amount of energy measured in microWatts per square meter (µW/m²) that will include high frequency EMF (100 kHz to 300 GHz) as used in wireless transmission (e.g. cell phones, computers, screens, TVs, cell towers, wifi routers, Bluetooth devices, etc.)
While there are a host of different standards for EMF exposure limits set by different organisations in different countries, these are generally based on thermal effects and accordingly the limits tend to be extremely high and not consistent with what is known about the harmful effects of radio frequency radiation. Examples include the limits set by the International Commission on Non-Ionizing Radiation Protection (ICNIRP) and those by the Institute of Electrical and Electronics Engineers (IEEE) through its International Committee on Electromagnetic Safety (updated in 2019).
ICNIRP has developed Exposure Limit Values (ELVs) and Action Levels (Als) for static magnetic and electrical fields and time-variable electromagnetic fields that have in many countries been transposed into law, especially to protect workplace environments – such as in the European Union and through the Control of Electromagnetic Fields at Work Regulations 2016 in the UK. These are limits for the amount of energy emitted by the EMF source and the resultant power absorbed per unit mass of body tissue.
Anyone concerned about electrosmog, has to disregard these levels because they are based only on thermal effects, despite intense lobbying by scientists and campaign organisations to include non-thermal effects. Not only that, humans and all forms of life are, each year, being exposed to an ever greater number of devices emitting human-created EMFs, including digital signals that are new-to-nature, that have been demonstrated to interfere with biological systems (see Henry Lai’s 2022 research summaries on the Bioinitiative 2012 website).
>>> Download Graham Arthur’s ‘Tips for Reducing EMF Exposure’ that was created especially to help people avoid becoming electrohypersensitive or to reduce symptoms of electrohypersensitivity.
All electrical and electronic devices sold on the European (European Economic Area, EEA) market require a CE mark. This mark affirms that the manufacturer has conformed to relevant European health, safety and environmental protection standards. That typically means conformity to European standards for electromagnetic compatibility (i.e. it meets the standards set in the EU’s EMC Directive (2014/30/EU), that applies across the EEA).
As a point of interest (and amusement?), given that so many electronic goods come in from China, some unscrupulous Chinese operators apparently have been known to illegally print the CE mark on their goods without ensuring conformity to relevant standards. These can often be identified by their use of the wrong fonts or character spacing and we were informed that among such disreputable companies there is the mistaken belief that ‘CE’ is an abbreviation of ‘Chinese Export’!
While you will find a CE mark on all but the most ‘wacky’ (read: potentially ineffective or dangerous) devices sold on the European market, the problem is that it is the manufacturer’s responsibility to conform to the relevant standards, and there is some debate as to which ones are relevant. Not only that, there are no specific standards for frequency-based devices directly relevant to their health application, causing some companies to make do by meeting the lowest standards, those required for general household electric and electronic goods.
The point is, it’s not easy doing due diligence when the framework for ensuring devices don’t cause harm is half-baked or rickety. Some companies comply with many more standards than others, many don’t specify exactly which ones they comply with, and some argue (incorrectly) that CE mark conformity means their device has been proven to be safe for its intended use. This isn’t the case necessarily, as, while EMC conformity might mean the device doesn’t emit levels of radio frequency radiation that exceed the ICNIRP standards that the directive is based on, it doesn’t mean the device is safe in its intended use as a frequency-based device.
This is the same problem we face with cell phones. The manufacturers tell us they’re safe because they conform to ICNIRP (that they’ve helped develop), but we also know (as discussed above) why these standards are grossly insufficient, hence the widespread and increasing problem of electrohypersensitivity. To understand safety, much more extensive evaluation is necessary, with due account being taken of dosimetry, itself a hugely challenging area.
So who’s your best friend?
For many it may indeed be a dog. But it’s OK to also have a technology partner – and let’s hope that’s not your cell phone! It’s a device many of us can use in order to better understand our exposure to the invisible and potentially harmful EMF smog we can all be surrounded by (especially from cell phones!) – often unknowingly. Yes, of course, I’m talking about an EMF meter.
There are many different makes and models available commercially, but I personally have found the highly portable, US-made Trifield TF2 to be particularly useful with a broad frequency range and good sensitivity. It measures magnetic (e.g. for powerlines, appliances, motors, wiring in walls, etc.) and electrical fields (e.g. for fluorescent lights, power outlets, switches, dimmers) in both standard and weighted modes (the latter means the readings become more sensitive in the mid-band), as well as the RF (radio frequency) range (e.g. for cell phones, computers, wifi routers, microwaves, radio/TV transmissions).
A Trifield device, or similar, can be fantastically helpful to better understand EMFs in your home and workplace. If you get high readings when measuring RF, magnetic or electrical fields in particular locations in which you spend a lot of time, there are often changes that you can make by moving equipment around or turning some of them off when they’re not in use. See Graham Arthur’s tips for reducing EMF exposure, mentioned above, for further information.
Trifield suggests the following levels might be reasonable thresholds for ‘EMF safe’ environments for the following three fields. Unlike the non-sensical ICNIRP limits, the company suggests these levels make sense because there is no evidence for the induction of health problems (even non-thermally induced ones) when levels are below them:
- Magnetic field: 3 mG standard, 5 mG weighted
- Electrical field: 50 V/m standard or weighted
- RF: 0.200 mW/m2 (field measurement), 1.000 mW/m2 (peak measurement)
Demystifying frequency devices
With our dining table set, having covered off some of the basics (let’s call the bit above our starter), let’s now dig into some of the technologies that are out there (prepare now for the main course).
The first step in my journey to help demystify the area got me building a ‘taxonomy’ of devices that covers some of the most common or popular types of devices that are available commercially. This journey took me through a significant amount of the published literature, but I found one journal article and one website to be particularly helpful in identifying frequency technologies that had been widely studied, some of them for over 70 years.
The journal article to which I was referring (and I’ve had the great pleasure of meeting one if its authors, Tiffany Barsotti) is as follows, along with the website:
>>> Electrotherapy on the web, compiled by the now-retired Prof Tim Watson of the Universities of Hertfordshire and Lincoln, a world renowned expert on electrotherapy. Prof Watson is also the author of the book Electrotherapy: Evidence-based Practice (2019, Blackwell), now in its 12th edition.
The taxonomy (inevitably incomplete as with most taxonomies of complex systems) is shown in Figure 4.
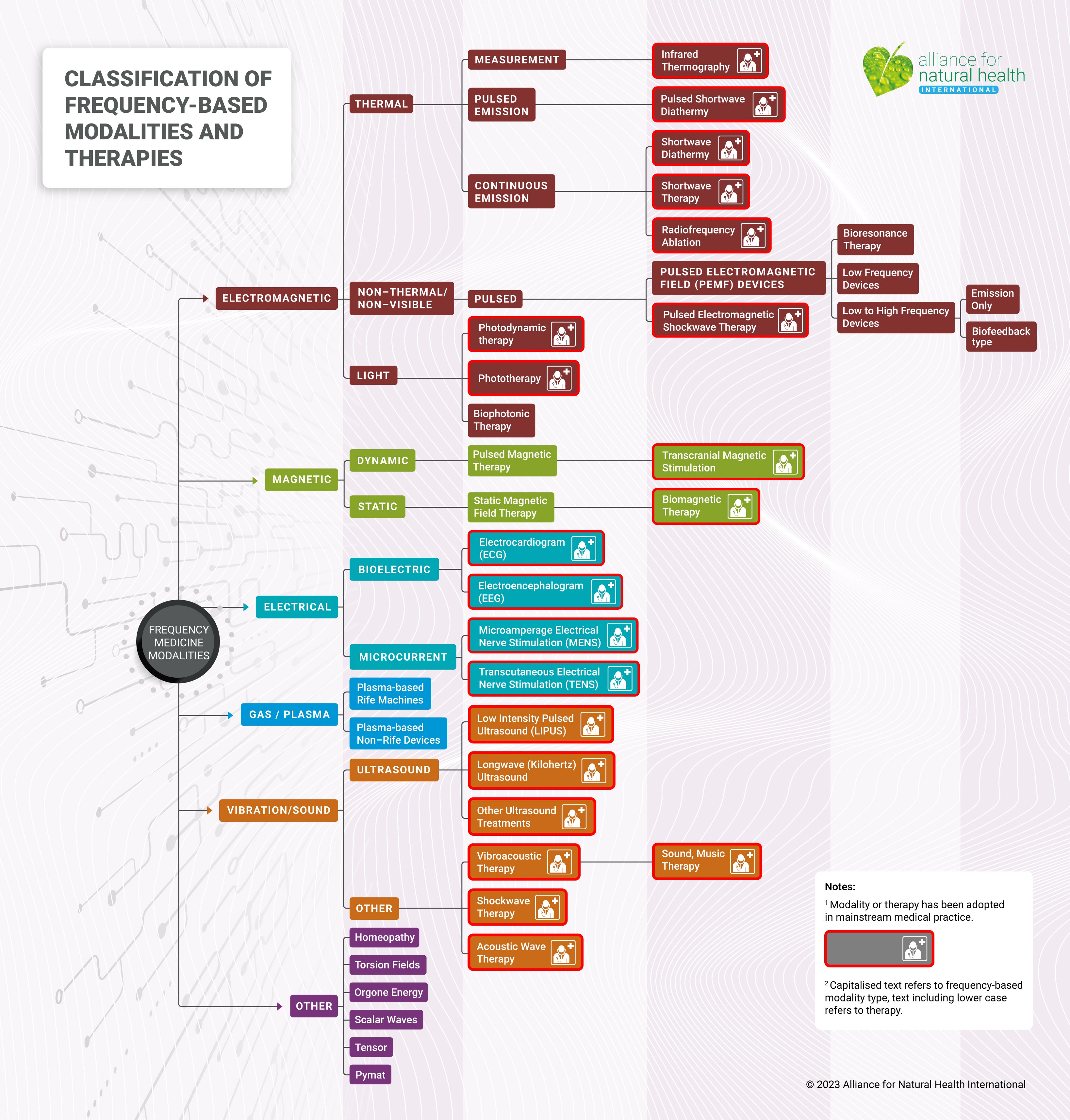
Figure 4. Non-exhaustive classification of frequency-based modalities and therapies (with therapy type/category given in brackets).
On building this classification, we were surprised at the number of frequency-based technologies that had already been adopted by the medical mainstream (not necessarily exclusively), especially in the fields of physiotherapy, neurology and dermatology (20 out of 31 = ~65%). Note that for each device type, there are often numerous different manufacturers.
This information gives you the capacity to immediately disregard anyone’s attempt to cast aspersions on frequency medicine if they try to claim it’s nothing more than fringe pseudoscience! The classification screams this is just not the case! And while we’re on this delicate point, let’s not be fooled into thinking pseudoscience has only ever been associated with alternative medicine – there’s bucket loads of it in mainstream medicine (more on that another day!)
But for us ‘believers’ in the power of frequency, here’s the horse pill we really need to swallow: frequency medicine has become increasingly accepted as the basis of diagnostic technologies, but it has made little impression in any of the areas where it might be used as a treatment for disease if it means it would then compete head-to-head with Big Pharma’s cash cows; think heart disease, cancer, infectious diseases, depression, arthritis, and diabetes. You’re unlikely to need me to explain why.
Entering the lion’s den
To unpack this next part of our journey, we need to enter the complex world of a partially regulated market that spans the continuum between the medical mainstream and the wellbeing sector, interfacing with the periphery of the most ‘out-there’ realms of alternative medicine (refer to Fig. 5 to view a selection of devices that were subject to our analysis).
We need to take on board the fact that the sector operates within a rapidly emerging scientific discipline in which there is still little general consensus, and, within it, are actors often keen to protect their intellectual property. On some occasions, you even get to encounter shameless and fanciful marketing of devices that are either known by their makers to not be what they claim, or, just as bad, the marketeers barely know anything about the technical specifications of what they are selling.

Figure 5. A selection of frequency-based devices used in conventional medicine and in the wellness space.
Key: A = BICOM Resonance Device (Pulsed Electromagnetic Field (PEMF) device). B = Shortwave Diathermy (Shortwave Diathermy, Continuous Emission). C = Homeopathy (Other). D = Magnetic therapy (Biomagnetic Therapy). E = Vitatec Vitalfield Devices (Global Diagnostics, Mito, DigiconPro) (Pulsed Electromagnetic Field (PEMF) devices). F = Phototherapy (Phototherapy). G = Rayonex Rayocomp PS 1000 polar 4.0 (Bioresonance Therapy). H = Resonant Light PERL (Plasma-based Rife Machines). I = Shockwave therapy (Vibration/Sound). J = Transcutaneous Electrical Nerve Stimulation (TENS) Machine (Microcurrent). K = Tensor Field Generator (Other). L = Low Intensity Pulsed Ultrasound (LIPUS) (Ultrasound).
Credits: A, BICOM Resonance Device; B, Shortwave Diathermy; D, Biomagnetic therapy; E, Vitatec Vitalfield; G, Rayonex Rayocomp PS 1000 Polar 4.0; H, Resonant Light PERL; K, Tensor Field Generator; L, Low Intensity Pulsed Ultrasound (LIPUS).
During our research for this article, we requested data on some specific technical criteria identified by a leading researcher in the field, Bulgarian scientist, Prof Marko Markov PhD. Prof Markov is author of more than 14 books, 192 scientific articles, and 282 papers and short communications given at various international meetings on the subject. Among his works, he is editor and co-author of the highly informative book, Electromagnetic Fields in Biology and Medicine (2015, CRC Press/Routledge).
In his 2015 paper titled ‘XXIst century magnetotherapy’ (Electromagn Biol Med, 34(3): 190-196), Markov stated:“The manufacturers and distributors of magnetotherapeutic devices, as a rule, do not provide sufficient information about the device characteristics. In most cases, it is not done on purpose, but because of lack of knowledge as to what information is necessary for clinicians to make proper selection of the device and protocol for treatment.”
In the same paper, Prof Markov goes on to list the parameters he argues are necessary “for characterization of device and study/clinical trial” – and accordingly, we have sought to solicit data on these parameters from selected manufacturers:
- Type of the field
- Frequency
- Pulse shape
- Intensity or induction
- Gradient (dB/dt)
- Vector (dB/dx)
- Component (electric or magnetic)
- Depth of penetration
- Localization
- Time of exposure (duration of session)
The replies we received from some companies from whom we requested information suggested there is a lack of knowledge or an insufficient desire for transparency.
One representative indicated its gratitude that we were writing an article, but added, “…we don't know how to provide the data you need.” Another said, “It's all proprietary information and I signed a non disclosure agreement so I can't provide you with technical specifications”. One couldn’t, or wouldn’t, provide any technical data, in the hope the following would be sufficient; “[our device] emits its own resonating frequencies which create a field.” Yet another said it would like to provide answers about its company’s device “…but those answers don’t really fall into the categories you’re asking about.”
The consequences of poor industry self-regulation aren’t good for natural health
There are five basic properties of any frequency medicine device that you should be able to readily know about from the outset, prior to using it.
Firstly, is the device able to measure all, or part, of the body’s biofield (energy body, see Part 1), and if so, what measurements is it taking from which parts of the body?
Secondly, does it emit or deliver frequencies to the body? If so, what are some of the important parameters of these signals?
Thirdly, does it contain any algorithms that change the frequencies that it delivers according to what it has measured? In other words, does it use some kind of a biofeedback system, and if so, are some details of it available?
Fourthly, what are the specifications that provide information on the quality of the device components that receive and emit electrical, electromagnetic or acoustic signals, and, if relevant, through what components are these signals transmitted (e.g. cables) or converted (e.g. digital to analogue converter)?
Fifthly and finally, can the company provide instructions on recommended use (including duration of exposure), as well as evidence that the device is safe, that people have benefited from its use? If so, are these data plausible and are they of adequate quality?
As frequency-based devices represent an emerging industry sector, technological specifications are varied in both type and measuring unit. If the device is emitting electromagnetic radiation with the expectation that it will modulate cell or tissue function, it is important that a user or practitioner is able to readily access information on frequency ranges, magnetic flux densities and dosimetry (how much of what type of radiation is delivered to the body). Given the complexity of some of the devices, these data will often need to be given in ranges, rather than as discrete figures.
For many companies this might seem a lot to ask, but would you buy a processed food at your local supermarket that chose not to specify the ingredients they’d used to make it? Would you buy a medicine that didn’t have a label? Would you buy a motor car that didn’t specify its performance or efficiency data?
Our sense is that if frequency device manufacturers as a whole don’t raise their game and put more information into the public domain as part of their responsibilities as a self-regulated industry, they will be forced, through the political process that is generally ambivalent about non-pharmaceutical approaches, into becoming regulated over time.
As we’ve seen from past history in the field of dietary supplements and other natural modalities, this is rarely a good thing either for natural health or for the wellbeing of people. Common outcomes of government regulation are: the knee-capping of choice, the elimination of the most innovative, smaller players, and preferential treatment of those with the deepest pockets who toe the mainstream line.
A particularly vulnerable area are those many PEMF devices (Fig. 4) in the wellbeing space which don’t currently have any medical device registration from a regulatory authority such as the US FDA, the UK’s MHRA, or their equivalents.
How do frequency-based devices work?
Let’s talk about measurements first. You can measure the human biofield in many dimensions, scales and resolutions, not unlike the way you measure or evaluate any other complex system, be it, for example, our planet, a lake, or an apple orchard.
Sometimes you want a generalised view, sometimes you want to get in close or dive especially deep. Sometimes you’ve got systems that give you a very high resolution, other times, the resolution you’ve got to play with is more generalised, or even fuzzy. Sometimes, even, the signal’s so weak and fuzzy you’re not sure if you can distinguish what you’re looking at from the background frequencies of natural and technological origin.
You may be dealing with equipment or components that have extraordinary levels of resolution, akin to when you use a macro lens on a camera that allows you to magnify the eye of spider such that it fills your computer screen. But use a telescope from a satellite to view the field you photographed the spider in, and things look very different. These kinds of differing perspectives and resolution capacities are part and parcel of different systems that attempt to measure the biofield.
But just like when you buy your camera, a potential buyer of a frequency-based device should have ready access to detail about the technology’s specifications and capacities. Currently, this is not always the case in this sector.
It's also worth remembering, even if you’re dealing with a highly sensitive, high resolution system that’s able to measure specific areas of the body, the measurements don’t necessarily translate directly to the physiology or pathology we’re used to dealing with when we look at the physical body and the underlying physiological and biochemical processes that function within it. While the precise mechanisms have yet to be elucidated or agreed upon through consensus, this is likely because the non-biochemical, energetic system of the body – the biofield – actually controls the other processes and operates in the realms of quantum biology, not Newtonian biology. Looking at it another way, the biofield is likely the master controller of the biological system; the invisible information matrix that is superimposed, both through and over, all living beings.
Some devices are restricted to low frequencies (say below 100 Hz), some manufacturers claiming that is because these are the ones the body operates with and they don’t interfere with the radio frequencies used in communication systems that are known to be harmful.
As the science progresses, it seems such views are increasingly invalid, as different parts of our bodies emanate an incredibly broad range of frequencies, from very low frequencies in the sub-100 Hz range, through the kilohertz (KHz), gigahertz (GHz), terahertz (THz) and even into the picohertz (PHz) range, and probably beyond. This is well illustrated in Fig. 6, taken from Kučera & Havelka (2012).
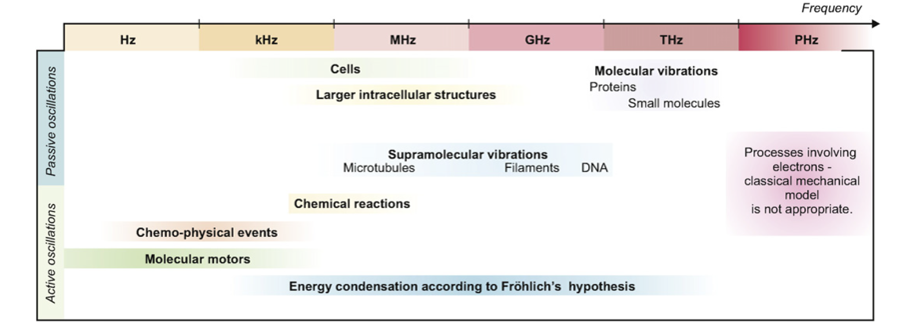
Figure 6. Spontaneous mechanical oscillations (passive and active) in different parts of the human body within the frequency spectrum. Source: Kučera & Havelka (2012).
Even the ultraweak biophoton emissions from DNA as explored by Fritz-Albert Popp and co-workers (see Part 1) are in the ultraviolet to visible light range (wavelength 200-800 nm).
Bottom line, whether or not the typically ultra-weak signals can or can’t be detected across the range is down to the sensitivity and specificity of the antennae being used. This is in effect a performance characteristic and an area that we believe should ideally be specified on consumer-facing specifications. Currently, such declarations are uncommon on many machines in the wellness space.
When it comes to frequency emissions, we open a can of worms. Much of the specification data appears to be guarded closely in order to protect intellectual property (IP). My sense is, nonetheless, that a lot more could be disclosed without risking IP. For example, disclosing certain characteristics of the emitted frequencies such as the frequency range, wavelength range and energy output range would still mean, for example, that details of the waveform, the pattern of any pulses, and the algorithms that control any biofeedback systems, would remain confidential. We were actually surprised, for the 23 devices we evaluated based largely on publicly accessible information, together with a prompt for any additional information by email, how few data fitting Markov’s checklist of parameters were available. However, there were clear exceptions. The data we managed to tabulate are shown in the Table below.
Table. Summary of publicly accessible information from a selected range of frequency medicine devices used in the health and wellbeing sector (scroll to right to view full table).
| Device brand name (manufacturer) | Device type | Registered medical device (Y/ N), class if relevant | Energy system measurement (diagnostic) (M) and/or treatment (T) | Frequency receiver (Y/N: if yes, incl range) | Electrically-powered frequency emission (Y/N, if yes, incl type e.g. PEMF) | Markov parameters* (for emission devices only) | Evidence of effectiveness e.g. trials (published, unpublished), testimonials – details) | Website |
|
ARC Microtech ARC4Health |
Transcutaneous Electrical Nerve Stimulation (TENS) | Yes, IIa | T | - | Y, microcurrent | Output current - 0-400 uA. |
https://arcmicrotech.com/ |
https://arcmicrotech.com/ |
| BICOM Optima | Pulsed Electromagnetic Field (PEMF) Devices/Bioresonance Therapy | Yes, IIa | M | - | Y, PEMF | 1 Hz to 250 kHz. | https://www.bicom-bioresonance.com/clinical-study/ | https://www.bicom-bioresonance.com/ |
| BioEnergetiX WellNES System | Pulsed Electromagnetic Field (PEMF) Devices (Scenar) |
N | M + T | Y, 15 – 480 Hz | Y, PEMF | None found/offered. |
https://www.neshealth.com/2022-university-research https://www.neshealth.com/en/nes-science-papers/ Patient testimonials: https://www.neshealth.com/portal-page-client-offer/ |
https://www.neshealth.com/en/ |
| Biophilia Tracker | Pulsed Electromagnetic Field (PEMF) Device | N | M + T | - | Y | None found/offered. | - | https://www.biophiliatracker.com/Biophilia-Tracker-X4-MAX |
| Bio-Well Gas Discharge Visualisation [GDV] camera and | Gas Discharge Visualisation (GDV) | N | M | Y | N | Not relevant (as non-emitting) | - | GDV camera: https://gdvcamera.com/gdvcamera-bio-well/ |
| Bio-Well Bio-Cor EHF | Vibroacoustic and Electromagnetic/Milliwave Therapy | N | T | Y, GDV camera | Y, Milliwave | Extremely High Frequency (EHF) in the millimeter gigahertz range with a very low intensity; wavelengths specified in two regimes: 1.8+4.0+7.7+8.2+9.2 and 4.9+5.5+7.8+9.5 mm; duration of exposure specified. | - | Bio-Cor: http://www.bio-well.com/ |
| Chiren 3.0 – Biophoton Light Therapy | Biophotonic Therapy | N | M + T | Y | Y, photon | Photons, 200-800 nm wavelength. |
http://www.biontology.com/research/ Testimonials: http://www.biontology.com |
http://www.biontology.com/biophoton-instruments/chiren-2/ |
| Energy Enhancement System (EES) | Other / Scalar | N | T | - | Yes, scalar | None found/offered. |
https://www.eesystem.com/research/ Testimonials: https://www.eesystem.com/ee- |
https://www.eesystem.com/ |
| Harmonic Egg Healing | Vibtroacoustic/Sound/Music | N | T | N | Resonates up to 1,200 Hz | Frequency range and exposure duration given (most other parameters not relevant to acoustic devices). | Testimonials: https://harmonicegg.com /about-harmonic-egg-bio-healing/testimonials/ |
https://harmonicegg.com/ |
| Healy Professional Edition | Pulsed Electromagnetic Field (PEMF) Device / Bioresonance type | N | M + T | N | Yes, pulsed, multiple set programs. | The stimulation output can be varied between -10 V and +10 V, 0 to 1 MHz, 0 – 4 mA. | - | https://eu.healy.shop/ |
| Holimed RemiWave Pro | Pulsed Electromagnetic Field (PEMF) Device / Bioresonance type | N | M + T | Y | Y, ? | 0–1,000,000 Hertz (1 MHz). | https://www.holimed.com/ eav-and-bioresonance-terminology-bioresonance-modes-a-and-ai/ |
https://www.holimed.com/the-bioresonance-devices-of-holimed/ |
| IteraCare Classic wand by Prife | Thermal / Non-thermal Terahertz wave | N | T | N | Y, continuous | None found/offered. | Testimonials: https://terahertz-device.com /iteracare-testimonials-reviews/ |
|
| Iyashi Zero Point Eenergy Wand | Other / (Scalar) (Subtle energy) | N | T | N | N | "Providing over 18000+ energetic frequencies" (frequency range unspecified) | Video testimonial: https://iyashisource.com /iyashi-zero-point-energy-wand-c-53_3 |
https://iyashisource.com/iyashi-zero-point-energy-wand-c-53_3 |
| Jellen Portable High Frequency violet ray machine | Plasma | N | T | N | Y | Up to 200,000 Hz. | - | https://www.jellenproducts.com/jellen-portable-high-frequency-machine-spa-grade/ |
| MORA Nova | Pulsed Electromagnetic Field (PEMF) Device / Bioresonance type | N | M + T | Y, 0.1 Hz – 1 MHz | Y, ? | 0.1 Hz – 1 MHz (Aid 0.1 – 1.000.000) | - | |
| Oberon Biofeedback Gold | Plasma-based Rife Device | N | M + T | Y, 5 - 30 MHz | Y | Low-frequency 240 Hz High-frequency 1.5-4.5 GHz |
- | https://oberondiagnostic.com/oberon/the-product/ |
| PERL M+ and ProGen3 by Resonant Light Technology | Plasma-based Rife Device with ~2000 frequency sets | N | M + T | Y, continuous or pulsed | Frequency generator with multiple programs that can generate sine, square or triangular waveforms, from 1 Hz to 4,000,000 Hz with accessories; from 1Hz to 300,000Hz with PERL M+. PERL M+ emits up to 300,000 Hz with 0.001 Hz accuracy, 27.120 Mhz with 1 - 1,000,000 Hz effective modulation; 11.05 m wavelength; amplitude 100 W peak to peak, modulated at targeted frequency; At a distance of 3m, energy output was 95.8dBuV. This translates to 1.008e-5 W/m2, 1.008e-6 mW/cm2, 2.065e-10 Tesla, 2.065e-6 Gauss at 3m. | https://www.resonantlight.com/frequency-101/ | https://www.resonantlight.com | |
| Qest 4 | Electromagnetic device | N | M + T | - | Y | None found/offered. | - | https://www.qest4.co.uk/ |
|
Rayonex Biomedical - - Rayocomp PS10 |
Pulsed Electromagnetic Field (PEMF) Devices | Y IIa | M + T | Up to 3 GHz | Continuous sinusiodal wave form; Frequency up to 3 GHz; wavelength can be calculated based on speed of light and frequency (specific number not available); Depth of penetration, no specific parameter available, but clinical prospective, double-blind randomised and placebo-controlled study showed that internal organs can be reached with Bioresonance according to Paul Schmidt; Localizaton, detectors made from a special cotton fabric in which very fine stainless-steel wires are woven; different sizes of detectors to allow placement on patient or patient can lie on it (in form of a fitted sheet); Duration fo exposure typically 60 minutes. | https://bioresonance.com | ||
| Sensate | VibroAcoustic Wave Therapy | N | T | N | Y, acoustic/vibratory | 20 - 140 Hz acoustic (other parameters not relevant). | https://buy.getsensate.com/researchstudy/ Testimonials on shop site: https://www.getsensate.com/products /sensate2 |
https://www.getsensate.com/products/sensate2 |
| Spooky2 Rife | Plasma-based Rife Devices, Scalar | N | M + T T |
- | Yes, PEMF | Up to 3.5 MHz. | https://www.spooky2.com/rife-machine/ Testimonials: https://www.spooky2.com/rife- machine-success-stories-testimonials/ |
https://www.spooky2.com/rife-machine/ |
| Vitatec Vitalfield Technology - Mito | Pulsed Electromagnetic Field (PEMF) Devices | N | M + T | Y, <1Hz to >10 GHz (into visible light spectrum) | Y, variable, 1 Hz to 120 GHz | Frequency: <1 Hz to 120 GHz, Pulsed, variable; Waveform variable (including triangle); wavelength 415 nm - 15 µm; Intensity/induction 1.5 mT; Gradient (dB/dt) 1.5 T/s; Electric and electromagnetic components; Depth of penetration from few mm to whole body; Exposure 15-60 min. | Testimonials: https://www.medtec.at/en/referenzen/ | |
| Vitatec Vitalfield Technology - Global Diagnostics | Pulsed Electromagnetic Field (PEMF) Devices | N | M + T | Y | 1 Hz to 120 GHz | Electric (capacitive coupling) field; Very variable emission pattern; Frequency 0.1 Hz to 1 GHz; energetic value < 400 mV; Depth of penetration whole body; Exposure 15-50 min. | Testimonials: https://www.medtec.at /en/referenzen/ |
* These are parameters identified by Prof Marko Markov “for characterization of device and study/clinical trial”, discussed above, and derived from Markov M. Electromagn Biol Med, 2015; 34(3): 190-196.
IMPORTANT NOTE: We have entered data in the above table that we have been able to find in the public domain or have received following requests to the best of our ability. This information is for guidance only and may be in error or there may be omissions. For that reason, we urge anyone interested in any of these devices to contact the manufacturer or distributor directly for any further information. In the event of any errors or omissions, we also would be very happy to hear from any of the manufacturers listed with the view to making any corrections or additions.
From this small sample of devices (Table), there is evidently great variation between the kinds of devices and technical data available about them. In the acoustic and vibroacoustic area, the data are obviously much more straightforward, so it is in the area of electrically-powered electromagnetic, plasma-based and scalar devices that emit electromagnetic frequencies where data become much more relevant.
There were clearly a few companies that have a much greater degree of transparency than others, the standouts being Vitatec, Rayonex, Bio-Well and Resonant Light Technologies (PERL+ and ProGen3). By contrast, there were other companies where standards of data transparency appeared to fall well short of expectations.
We have some concerns over devices that are heavily marketed on the basis of testimonials, with little technical detail. The iTeraCare wand was one such example, where the device is categorised by the manufacturer (presumably owing to CE mark certifications) as a "hot air blower", yet details about the claimed terahertz electromagnetic radiation output don't appear to be available in the public domain. Claims by multi-level network distributors who are selling the devices, including to those who are seriously ill with C19 'vaccine' injury, vary, some suggesting the waves penetrate 20-30 cm into the body, others 20-30 mm. Contact details or a website for the manufacture was difficult to find, not to be confused by the network marketing company Prife International that has exclusive distributorship.
Other devices, such as the Energy Enhancement System (EES) that relies on scalar energy typically issued through batteries of computer screens is being pushed hard by influential individuals including many integrative doctors in the USA. While some of the case reports are inspiring, we were surprised to find little in the way of technical detail about the underlying technology.
Clean or dirty signals?
There are many things about various devices that can’t be revealed by reading the manufacturers’ specifications and marketing materials, even if they appear quite comprehensive.
Take, for instance, the nature of transmitting signals received by the body from an electrode of some form, reading or interpreting them in a read-out of some sort on the device, and returning different signals via an algorithm in ways that modulate the body’s response with the aim of improving energetic coherence and function. This is, after all, the principle aim of many devices in the wellness space.
You’ll recall that the electromagnetic (including photonic) signals emitted by the body are very (even ‘ultra’) weak. That doesn’t make them unimportant; it probably makes them more important, but also more able to be interfered with by human-created electromagnetic signals used (also) for communication purposes.
The body’s signals work across a full harmonic range from very low to very high frequencies – like an orchestra. Just like you can only hear a fraction of the full range of acoustic sounds, harmonies and resultant harmonics produced during Karajan and the Berlin Philharmonic’s rendition of Mahler’s 9th symphony when you listen to it through a ghetto blaster, much of the signal quality can be lost if the receiver (electrodes or antennae) are lacking in quality and there is excessive loss and noise when the signals travel between the body and the device itself. By contrast, a highly sensitive receiver, with little loss in quality of signal transmission, that is capable of a wide frequency range, allows you to ‘listen’ to the information emanating from the body’s electromagnetic field in its full glory. With all the harmonics in place, even the likes of Mahler might have been appeased had he been alive to ‘hear’ the human body.
In many cases, long cables (3 metres or more in length) are used by manufacturers to allow the cables to reach a patient or client lying prone on a couch. But what is the quality of these cables? And what is the quality or sensitivity of the antennae or electrodes? We know in some cases, these are excellent, while in other cases, this appears a lesser priority. So how does a practitioner or potential user know whether a manufacturer has used the best sensors available and the highest quality, double or triple insulated cables specifically designed for very low voltages, if this information isn't made publicly available?
What also happens to signals emitted from digital devices? Do they emit step-like, digital signals that are alien to natural systems prior to the invention of digital communication systems? Have they been converted via a digital to analogue converter (DAC)? Has the conversion happened without loss of key information?
Not sorting out these ancillary elements is akin to trying to drink an exclusive wine from a used Starbucks cup with the dregs left in it. And if you use the best technology to get the highest quality biological information and signalling you can get – presumably it makes sense to communicate this to potential buyers so they know they’re going to be drinking from a beautiful crystal glass deserving of their biofield?
Do frequency medicine devices work?
This is probably the toughest question to unravel for a potential user. There are many different ways that people make a judgment over whether a device works, in the sense it enhances the body’s natural homeostatic or healing mechanisms. Here are 10 possibilities:
- Personal experience
- Word of mouth
- Public-facing testimonials
- Key opinion leader or influencer’s communication or endorsement
- Advertising, along with claims, which may or may not be substantiated
- Third party reviews published in the popular, special interest or scientific media
- Mechanistic studies by the manufacturer or third party that demonstrates a plausible mechanism for a beneficial biological effect
- Manufacturer’s own outcome-based/effectiveness trials, ‘unpublished’ (typically produced as a non-peer reviewed report) or published in the peer reviewed literature
- Outcome-based/effectiveness trials or study by a third party (independent institution or company), ‘unpublished’ or published in the peer review
- Aggregated clinical evidence i.e. evidence of consistent positive health outcomes associated with the use of the device by multiple practitioners and many more patients.
One of the results of our own evaluation of this sector is that there’s a lot of smart marketing out there, but, for some devices, the substance (read: data) we’d hoped to see just wasn’t available. This is much less the case for those devices that have been adopted by the medical mainstream (Fig. 4) and others that have received Class IIa medical device registration for specific indications, such as the bioresonance devices by Rayonex and BICOM. This is because device registration requires proof of both safety and clinical effectiveness via clinical trials. This, however, does not mean that devices for which there are more data are necessarily better, more effective or even safer than those devices for which fewer data are available. It just means, as Dr Markov alludes in his 2015 paper, that it is not possible to make a meaningful assessment of the technology where crucial data, say on factors such as frequency and amplitude ranges, field gradient and duration of exposures have been designated by manufacturers.
The issue of data transparency and the need, or otherwise, to seek registration, is a complex one, in part because of the diversity of signals and fields with which different devices work, and because some devices work so much more holistically than others, on so many aspects of the physical body and biofield. This makes it much harder to squeeze them into the square peg format required for registration, that requires a clinical trial focused on given indications or health conditions.
But it’s not just that. Some manufacturers take a principled position of not wanting to disclose technical information to a regulatory authority given the well-known revolving door between drug/device regulators and Big Pharma. Others consider themselves as only making or marketing wellness devices designed for healthy people who don’t have serious diseases, so medical device registration isn’t appropriate. Others, still, would much rather keep their heads below the parapet, as they know only too well that the operating principles of their devices, involving the human biofield, are so alien to any regulator steeped in the biochemical, Newtonian-Cartesian model of medicine, that pursuing regulatory approval would almost certainly be fruitless. That is, until such time that regulators are forced to catch up with the emerging science on biofield devices.

Interacting human biofields — invisible to most, detected and measured by a rapidly increasing number of frequency-based devices
What to do…..nothing, or something? Our view is that the sector, as a whole, could do somewhat better at metering out relevant information to the public – to maintain the all-important bioethical principle of informed consent, as well as to support the notion, that’s been at the heart of ANH’s work since our beginnings over 20 years ago, of informed choice.
For some companies, lesser reliance on testimonials and advertising claims that cannot be independently substantiated would be a good start. So would collaborations with highly experienced and influential clinicians, who can then communicate their own findings from case reports or observational studies to peers. Collaborations with independent scientists in order to aggregate relevant clinical data so we can better understand effects within a science-based context would be a huge asset.
The use of spurious claims that are not possible for a practitioner or interested member of the public to corroborate, is no help to anyone in the long-term, not even to those whose companies might benefit from the short-term win such claims can bring. They simply give regulators – even non-government, self-appointed ones like the UK’s Advertising Standards Authority, a reason to sharpen their knives, as seen by this advisory, including two negative rulings on marketing claims for bioresonance therapy.
Much of this transition, no doubt, will come in time as the sector matures. The limitations of what is out there, in the public domain, are to a large extent just a symptom of the youthfulness of this rapidly emerging sector. All of it is made more confusing because the principles on which biofield devices operate are alien to so many, especially outside the German-speaking countries that have been the main hot bed of research of development to-date.
Asking if frequency medicine works is not a dissimilar question to asking if natural – or even pharmaceutical – medicine works. Of course it does! But this doesn’t mean it works in all people all of the time! It depends on multiple factors, including which devices, which element of human health you’re considering, under what conditions, on which person, at what time.
Now, some good news! In general terms, it’s not hard to find plenty of evidence of positive, beneficial effects, with an absence of any safety problems. But the evidence that some devices have been proven to work for some conditions and some people doesn’t mean this claim can be brandished across all those devices, including those that haven’t engaged in a more scientific process of evaluation. Imagine how the public would react if drug companies relied on the research studies on natural monacolins from red yeast rice to help sell their statin drugs! (Ouch – of course, some do!)
OK – now you want the detail. As the areas is so huge I want to point you to three useful reviews that link to many successful research studies and clarify the potential of frequency-based devices. These are as follows:
- Electrotherapy on the web
- Muehsam et al. 'An Overview of Biofield Devices' Global Adv Health Med 2015; 4 (suppl): 42-51
- ‘XXIst century magnetotherapy’ Electromagn Biol Med, 2015; 34(3): 190-196.
Despite the sometimes patchy picture of information currently available in the public domain, when one looks in totality at all of the available information and data, and considers the forces that this sector is up against given the monopolistic agenda of Big Pharma, I don’t for a moment doubt Einstein’s prediction that, “Future medicine will be the medicine of frequencies”.
One thing is for sure, the sector is growing. This trend tracks alongside the ever more widely recognised problem: the prevailing biochemical, molecular, genetic and Newtonian-Cartesian concepts that underpin mainstream, allopathic medicine are just too limited to deliver consistent, high quality healthcare.
More than that, an ever growing number of people are opening up to the idea that electromagnetic energy, frequencies and resonances are – as we discussed in Part 1 – essential to life. More interest results in more experiences, which means more devices sold, leading, in turn, to more research. As such, each year, the evidence base, particularly from all-important clinical practise, is expanding.
There’s another key reason for the mounting interest in frequency-based devices. As our bodies get ever more distorted by human-created electromagnetic fields, the importance of bringing them into coherence through the use of specific electromagnetic fields will become ever more important.
Conclusions
As an independent scientist, it has been something of a bumpy journey investigating the publicly available data and information being used to market frequency-based devices. Having said this, my enthusiasm over the potential for the frequency medicine sector to not only become central in the area of diagnostics, but also in treatment (both preventative and curative), has not been dampened in the slightest. I don’t doubt it will happen, because, like many, I fully acknowledge that frequency and electromagnetism is the next major frontier in medicine – because it is so fundamental to all biological processes.
What I am less sure about, however, is the time it will take to become universally accepted. This, in my view, will depend a lot on the investment technological leaders make in proving benefit and safety, the commitment shown to transparency and the degree of care and responsibility taken in communicating information and knowledge to the health professions and the wider world.
This also means navigating the regulatory swamp that has been created over some 70 years by the drug regulators who have established a system that works well for their paymasters, and has been deliberately orchestrated to shut out, or shut down, competition that might negatively impact the bottom lines of Big Pharma or Big Devices (have I just invented a new term?).
The nutritional and supplements industry is a case in point, having been at loggerheads with regulators for decades. But the science used to defend nutrition is still largely based on the biochemical model of physiology – and still ignores the electromagnetic components, resonances and quantum signalling that occurs when food and nutrients interact with the physical and energetic body.
Like with any new industrial sector, responsible self-regulation is the best way of avoiding the kind of events, however trivial they seem, that regulators will happily use to annihilate new competition. The over-zealous and entirely unnecessary actions the FDA and EU regulators have taken to knee-cap the rapidly expanding cannabidiol (CBD) sector, are cases in point.
Our appeal
As an alliance of natural health interests, with our primary mission being focused on benefiting people and preserving our right to natural health, we are keen to work with a group of leading players in the frequency medicine sector to facilitate the carving out of a framework for the responsible and sustainable development of the sector.
We invite scientists, researchers and company representatives within the frequency medicine or wellness technology sector to contact us at [email protected] if they are interested in co-creating a framework for this incredible, and exciting new frontier of medicine and wellness.
>> Feel free to republish - just follow our Alliance for Natural Health International Re-publishing Guidelines
>>> If you’re not already signed up for our weekly newsletter, sign up for free now using the SUBSCRIBE button at the top of our website – or better still – become a Pathfinder member and enjoy benefits unique to our members.
>>> Return to the homepage



Comments
your voice counts
03 February 2023 at 7:19 am
An excellent paper, cogent and easy to follow, thankyou.
I have used VEGA / WEGA for nearly 40 years and found it the most efficient and accurate of diagnostic tools,
well supported by research as well as practical experience. eg found prostate cancer in a chap who had been declared clear by the hospital , who on deeper examination , after the VEGA test, was found to have low grade cancer. You do not evaluate VEGA / WEGA in your paper ?
I have been a qualified acupuncturist for 44 years and Homoeopath, both classical and German complex systems for 41 years. I have treated just short of 30,000 patients in that time.
If we start with a common premise that disease starts in the "Energy" and works it's way down to the Physical
system, with the exceptions of direct viral / bacterial or fungal infection , then we are left with trying to shift something which has moved from Energetic to Physiological to Pathological.
I contend from experience that once something has become pathological that you need to do something direct as well as working on the Energy side.
A common example would be breast cancer , if you have a malignant lump , cut it out and then work on the
"Why did I get this , ? Why was my Energy system not sufficient to protect me ? What can I change about myself to alter my cellular system ? afterwards !!!!!!!!
06 February 2023 at 11:32 am
Many thanks Chris - yes VEGA as an electrodermal method didn't make it onto our list, like so many other devices, as it was just a small selection. And of course there are all the other Reinhold Voll based electrodermal testing companies that have modernised the process of allergy/intolerance testing including BEST, Quantum, LISTEN, Dermatron, etc. More another time! Thanks for your input. Best, Rob
03 February 2023 at 1:50 pm
Hi Rob
Thanks for the detailed analysis, certainly food for thought.
Anecdotally, we tried a TENS machine to see whether it would help us, but didn't find any benefit.
Given the way, the mind body works, I'd be surprised if Frequency Medicine doesn't have a part to play.
It would seem that part of the challenge is to determine a real connection with an ailment or well-being and testing for it. How on earth one would exclude all co-founders is beyond me.
The placebo effect is hugely powerful and in my view underestimated. So, even a machine that in reality does nothing will seem to work (at least for some).
Cheers
04 February 2023 at 12:08 pm
It's a great article, so thanks to Rob and ANH for bringing some definition. Here are some observations based on interactions with perhaps 1000 or so practitioners using various devices over the last 15 years, mainly referring to the more subtle end of the spectrum rather than the pure 'frequency medicine' devices.
Practitioners look at the device, and start by asking about all kinds of technical parameters, then over time, like Chris Boardman above, recognise that, in their hands, the device is 'accurate', 'effective' etc. Some practitioners continue to look for the next technically 'superior' device, while others would not dream of letting their current system go.
Its also observed that any given practitioner uses their device in a specific manner which develops into grooves over time, and that will be quite different to how another practitioner uses it. The manufacturer's meanwhile, under-emphasise this aspect.
At the more subtle end of the spectrum (things that might be called 'biofield' devices), there is no doubt for me that trying to separate the practitioner from the device in studying the effectiveness, will not proceed very far.
It seems to become more a question of which system have you 'bonded with', and how much have you committed to making it work with and for you ? Of course that sounds wacky to a purely materialist reader.
The Muehsam paper referenced states as follows: "A more comprehensive theory of mind is required to under-stand nonlocal interactions and to further understand the biophysical bases for these effects. At this stage, models based upon quantum correlations appear promising,54,169 but testable hypotheses are needed in order to develop a more detailed functional framework. Development of the interfaces between physiology, biophysics, and a testable nonlocal theory of the role of the mind will elucidate the specific ways in which devices can be developed for detection and manipulation of biofield interactions."
The assumption in the first sentence above that there are 'biophysical bases for these effects' is an example of reversing the direction of causation that modern physics is quite loudly hinting at, and most societies have arrived at in history - that causation runs from conscious intention to matter and not vice versa. The implications of fully embodying that world-view in a materialist society are quite profound though, and those who have recognised it tend to end up rather 'off-grid', and do their later work without any tools, in ways that materialists find it hard to give credit to.
Some of them though, have left some interesting devices for us to help climb that ladder of deeper awareness, and indeed they seem to serve that purpose quite well, particularly when they provide scope for the practitioner's own creativity inside the therapeutic relationship with the client.
It is of course interesting to study and try to draw conclusions about the capabilities of different technologies, but as Muehsam says, without a theory of mind, the studies quickly run out of road. I recommend everyone who wants to understand this field to start with at least 50% of their research in the non-mental sphere represented of meditative and transcendent methods including body-consciousness. Too much of the mental study tends to make us reject powerful things too early, while too little, can indeed make us prone to believe anything the marketers say.
06 February 2023 at 11:14 am
Mark - thank for this very insightful comment. Yes - despite the 8,000 words - I've only scraped the surface of this huge area. But totally concur the notion that nonlocal effects and consciousness are likely at the heart of where frequency medicine needs to go as the field matures. My sense is that there will be a split between those technologies that still largely look at the body as a biochemical/bioenergetic system, and those that move to the higher/deeper levels associated with the link between energy, consciousness and the physical body/mental construct. Might you be interested in writing a piece for our website? Best, Rob
08 February 2023 at 6:26 pm
Yes, I'd be happy to give it a go.
05 February 2023 at 5:56 am
Dear Dr Verkerk,
I would prefer to discuss this with you personally, as all you post here relates to high end frequencies and sine waves which are not compatible with the human cell. They may have some short term benefit in pain relief, but if used in the long term will cause chronic fatigue of the cell, and reduction in the function of the immune system.
My Late husband Dr Bob Grace PhD ( Oxford University 1998) and I as working with him over 50 years in the field of magnetic resonance in relation to the human body found that a gentle oscillating microvibrational frequency is far more effective, and over a period will help the cells to maintain their elasticity and strength.
Bob worked along with doctors and scientists during these years both overseas in these years, and the results with a low band of frequencies did help people in a diseased state. our products have frequencies ranging from 0.5 hz through to 18 hz . The frequency band is 0.5 hz, 2hz,3hz,4 hz 5hz, 8 hz 12 hz 15 and 18 hz.The high ones are only recommended for sports warm ups and particularly with racing animals such as Greyhounds and horses. Bob was poisoned along with 4 other scientists at a conference at the TGA in Australia in 2005, and passed away after having lost both legs, eye sight, and complete paralysis of the rest of his body in that time. Please be free to email me as it would be wiser and easier to clarify his research.
The company currently operates out of the UK (www.magnacares.com, but as you would be aware, we are very restricted with what we can say. The claims made by the most on the internet media today because yes, they are motivated by money, and I certainly question almost all of the claims made by the owners and their clients. Sincerely, Avenel Grace. B.E.M.C (Bio-Energetic Medicine Consultant- Integrative School Of Medicine 1994, ) C.M.T.A ( Dip) Western Australia college of Magnetic energy medicine 1993. Certified Practitioner Of magnetic medicine (Australian Natural Therapies/ Tafe S.A 1994 ).
06 February 2023 at 11:21 am
Dear Avenel - I am sorry for your loss, what a tragic death your husband faced - and stunned to hear the poisoning occurred at a TGA conference. I'd be delighted to link up find out more about your and Bob's research that clearly focuses on the ELF/Schumann range. I will email you. Best, Rob
01 March 2023 at 12:54 am
Great job! This is a very exciting time. People need to be more discerning and intuitive about what energy modalities they use. There is no one size fits all. I have seen so many harm themselves with subtle energies. Education is key!
24 May 2023 at 7:49 am
I know you generally don't allow commercial links but drpawluk.com has a lot of free info on primarily the pemf devices. He does sell devices and has comparisons and free consultations available. I have no commercial interest in his site, I have just found him to be knowledgeable and the website to be helpful.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences