

Content Sections
By Rob Verkerk PhD; founder, scientific and executive director
Topline
- Omicron is being used by governments and health authorities to mandate or coerce ever more people into receiving covid-19 jabs
- It is imperative that sufficient information is given to potential vaccinees to allow properly informed consent. This article reviews key information that is not widely reported by governments, health authorities, vaccinators, the mainstream medical profession or the mass media
- Given that the most commonly used covid-19 jabs rely on providing genetic information to the body to force it to produce a modified form of the spike protein, the jabs should not be represented as ‘vaccines’
- The mRNA jabs rely on genetic material that is significantly altered to generate mutant spike proteins that retain their prefusion conformity even after they get into cells. The lipid nanoparticles have not been adequately studied for their safety.
- The viral vector jabs by AstraZeneca and Johnson & Johnson rely on human foetal cell lines and the majority of the protein in the jabs may be from this source, rather than from the viral vectors themselves
- The spike protein is toxic in its own right and may induce adverse effects on the body whether it is generated from genetic information from jabs or from naturally-acquired infection
- Contaminants, deliberate or accidental, have been found in many vial specimens
- There are no substantive data to justify the ‘safe and effective’ claims often made for covid-19 jabs, especially not in the face of omicron
- Covid-19 jabs, especially if given repeatedly every few months, will likely cause lasting negative impacts on immune system function so increasing the risk of a wide range of other diseases while increasing risks of adverse reactions
- Clear evidence has emerged that data used for ‘vaccine surveillance’ by the UK Health Security Agency (formerly Public Health England) has been accidentally or deliberately misrepresented to infer outcomes among the jabbed are better than for those who decline
- There is little or no evidence that informed consent is being, or has been, offered at any time during the ‘pandemic’.
Before diving into the detail, here is Rob's short, 10-minute video summary:
>>> Share link for video: https://odysee.com/@ANHInternational:5/Jab:b?r=qiRpRqU6X8oQNpqNBfwzZPqtyAwiRczS
Freedom on trial
Liberalism in Europe is not only under threat. It has in some parts already been extinguished. As the first European nation to mandate covid-19 injections, Austria will criminalise those who refuse the injections. Germany has since followed suit. Greeks will need to pay their government a monthly fee of €100 every month if they remain jab-free. On Monday night Queensland-based medical doctor, Robert Brennan, told those of us attending the weekly World Council for Health meeting that doctors in Australia who are de-licensed for speaking out about lockdowns, testing or injection risks will be criminally charged for impersonation if they continue to use their doctor title. We also heard more about the quarantine camps that are being set up, how indigenous populations are being targeted and how sacred sites are being destroyed under powers granted by the supposed ‘emergency’ status.
Layered over all of this is the emergence of the new SARS-CoV-2 variant, omicron, that is providing authorities in Europe and North America further justification to mandate or coerce people to be jabbed, most notably with so-called ‘boosters’ (presently existing stock of injections based on the original Wuhan strain, Wuhan_Hu-1). Much hype is being generated by emerging evidence of omicron’s superior transmissibility compared with delta.
Policies designed to increase ‘vaccination’ coverage and re-injection of previously injected people (use of ‘boosters’) are not based on any conclusive data or even mechanistic evidence on the likely effectiveness of this strategy. Instead, they rely on now outdated data from Israel (here, here and here) and England that an mRNA booster jab can reduce the chances of people getting severely ill if infected.
Such data are entirely irrelevant to a situation we might be in in the coming weeks if omicron becomes dominant. That’s because it is increasingly clear that the vaccinal antibodies elevated by the jab do precious little to protect people, given that omicron’s multiple mutations in the receptor-binding domain of its spike protein prevent the antibodies from neutralising it.
With all the coercion around us it is more important than ever that people really understand what the jabs are and how they work. We now know a little more about them compared with when they were first released on the public, so let’s have a closer look.
We will restrict our discussion to the two main types of ‘vaccines’, the mRNA and non-replicating viral vector types, respectively, that include 5 of the 8 WHO-approved covid-19 injections (Table 1).
Table 1. WHO approved covid-19 injections
|
Type |
Company |
Name |
No. of countries where WHO approval granted for emergency use |
No. of trials/countries |
|
mRNA |
Pfizer/BioNTech |
BNT162b2, Cominarty |
112 |
46 trials/21 countries |
|
Moderna
|
mRNA-1273 |
79 |
33 trials/8 countries |
|
|
Non-replicating viral vector |
Oxford/AstraZeneca |
AZD1222, Vaxzevria |
127 |
50 trials/23 countries |
|
Janssen/Johnson & Johnson |
Ad26.COV2 |
85 |
16 trials/18 countries |
|
|
Serum Institute of India |
Covidshield (Ox/AZ formulation)
|
47 |
2 trials/1 country |
Source data: COVID-19 Vaccine Tracker
Why the covid-19 jabs shouldn’t be described as ‘vaccines’
In a recent video I explained why the main contenders (mRNA and viral vector types) should not be described as ‘vaccines’ as they don’t meet the World Health Organization’s definition of being the administration of “agent-specific, but safe, antigenic components that in vaccinated individuals can induce protective immunity against the corresponding infectious agent.” That’s because both these jab types don’t actually contain any antigenic components. They contain genetic information that forces the body of the vaccinee to make antigenic components, namely the spike protein of the now no-longer-circulating Wuhan strain of SARS-CoV-2.
This is succinctly put by two eminent Austrian vaccine scientists from the Medical University of Vienna, Franz Heinz and Karin Stiasny, in their detailed review paper in a Nature journal, NPJ Vaccines, where they state that both types of ‘vaccine’ “...do not contain the spike protein but provide genetic information for its biosynthesis in body cells of the vaccine.”
The US Centers for Disease Control and Prevention (CDC) chose to revise its definition of a vaccine on 1 September 2021 so the mRNA and viral vector jabs wouldn’t fall foul of it. The vaccine definition changed from, “A product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease” to the broader, more inclusive definition, “A preparation that is used to stimulate the body’s immune response against diseases”. Other health authorities will undoubtedly follow suit as these new platforms become more and more widely used, and not just to target this one pathogen.
Such is the ‘let’s make it up as we go along’ approach, we noticed, at the time of writing, the CDC has failed to update the ‘vaccine’ entry on this glossary.
In their comprehensive review, Heinz and Stiasny refer to both the mRNA and viral vector type products as ‘genetic vaccines’ – because they deliver genetic information to the body to make it synthesise the antigen. This is why the term ‘gene therapy products’, while having been branded repeatedly as conspiracy theory, is a reasonable description. A paper published in the journal Genes and Immunity states that covid-19 ‘vaccines’ “...signify a breakthrough in the field of gene therapy, which has battled to achieve ordinary acknowledgement due to a large number of sceptical and conservative scientists and other claimed safety and translational concerns”. The ‘vaccine’ tag could be viewed as particularly misleading given the products are not capable of generating herd immunity as they don’t illicit a strong enough sterilising response from antibodies to prevent infection and transmission.
Furthermore, and contrary to what is inferred by health authorities, comprehensive research using a pseudovirus that expressed spike protein in Syrian hamsters conducted at the Salk Institute found that the spike protein (Fig 1) was far from harmless. It appears to be toxic in its own right and it is the primary component that induces the vascular disease that develops in severe, life-threatening cases of covid-19.

Figure 1. The spike protein of SARS-CoV-2, coated in sugar molecules (glycans), with receptor-binding domain in the upper, S1 subunit. Source: Nature, 2021
What might be in the vials that isn’t declared?
The simple answer is we don’t know. We know what we’re being told is in them, but there is increasing evidence of big variations in the quality and composition of different batches, which may or may not be deliberate. Contaminants, described in mainstream media articles as “black particles”, have been found in Japan (here and here), as has “white floating matter” in the Pfizer jabs.
There has also been considerable speculation around the presence of other materials that do not appear on the official data sheets, notably reduced graphene oxide (rGO), in the injection products. Graphene is a single atom thick layer of bonded carbon atoms arranged in a hexagonal pattern.
It has many remarkable properties and has been extensively researched for its ability as a potential vaccine carrier and adjuvant.
Dr Pablo Campra from Almeria University in Spain published a report (English translation on Researchgate here) on 2 November 2021 claiming the detection of graphene in the Pfizer ‘vaccine’. An interim report of the study be found here and a video and more information here.
One group of anonymous scientists that appear to be based in Germany, also reported at a conference finding graphene oxide in samples of all 5 of the WHO-approved ‘vaccines’ considered here.
Contesting these highly controversial views are fact checkers and mainstream news channels galore, as one would expect, but no serious analytical chemists.
Other than potential contaminants or hidden ingredients, there is also the possibility of being injected with nothing other than saline, as reported here, here and here).

What should be in the vials?
Let’s now look at what should be in the two types of ‘genetic vaccines’, summarised in Table 2.
Table 2. Claimed key ingredients in the 5 main WHO-approved covid-19 injections
|
Type |
Company |
Name |
Eukaryotic production |
Dosage |
Other key ingredients |
|
mRNA |
Pfizer/BioNTech |
BNT162b2, Cominarty |
N/a |
30 µg RNA (2x) |
|
|
Moderna
|
mRNA-1273, Spikevax |
N/a |
100 µg RNA (2x) |
||
|
Non-replicating viral vector |
Oxford/AstraZeneca |
AZD1222, Vaxzevria |
HEK293 |
5×1010 adenovirus vector particles (2x) |
Polysorbate 80 (E 433), sucrose, disodium edetate dihydrate |
|
Janssen/Johnson & Johnson |
Ad26.COV2 |
PER.C6 |
5×1010 adenovirus vector particles (1x) |
2-hydroxypropyl-β-cyclodextrin (HBCD) Citric acid monohydrate, Ethanol, Polysorbate-80 |
|
|
Serum Institute of India |
Covidshield (Ox/AZ formulation)
|
HEK293 |
5×1010 adenovirus vector particles (2x) |
Polysorbate 80 (E 433), sucrose, disodium edetate dihydrate |
*Pfizer/BioNTech (Cominarty) contains: ((4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2-hexyldecanoate, (ALC-0315), 2-[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide (ALC-0159), 1,2-Distearoyl-sn-glycero-3-phosphocholine (DSPC)
†Moderna (Spikevax) contains: Lipid SM-102 (heptadecan-9-yl 8-{(2-hydroxyethyl)[6-oxo-6-(undecyloxy)hexyl]amino}octanoate), 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC), 1,2-Dimyristoyl-rac-glycero-3-methoxypolyethylene glycol-2000 (PEG2000 DMG), Trometamol, Trometamol hydrochloride
mRNA type
Both the Pfizer and Moderna jabs rely on similar technologies, namely mRNA (messenger RNA) that is a transient intermediary between genes and proteins. Companies like Moderna have been founded to exploit the potential to use this technology to get the body to produce an array of therapeutic proteins.
The Moderna jab relies on over three times as much mRNA as that of Pfizer. The messenger RNA (mRNA) is synthetic and now commoditised, encoding instructions that force the vaccinee’s cellular machinery to produce a modified form of the full-length SARS-CoV-2 protein.
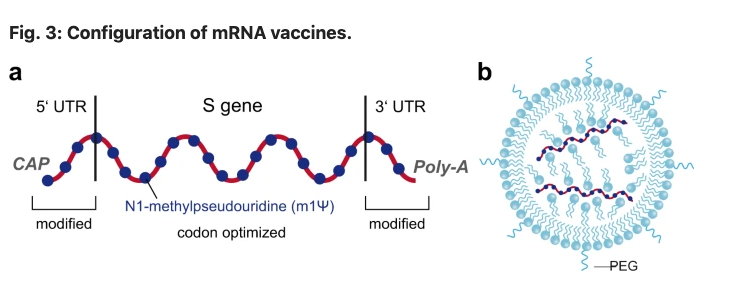
Source: Heinz FX, Stiasny K. npj Vaccines. 6, 104 (2021)
The RNA sequence in each of the two mRNA ‘vaccines’ is modified from the one used by the actual SARS-CoV-2 virus when it co-opts particular organelles in cells (endoplasmic reticulum and ribosomes) to translate the RNA that is converted to DNA to make its own spike proteins. The uridine bases are all substituted for N1-methylpseudouridine to make the mRNA both evade the immune system and enhance protein production. The RNA strand is also ‘capped’ and ‘tailed’ with methylguanosine and poly-adenine, respectively, to further stabilise the mRNA and promote its translation. The genetic instructions have yet another trick in store that’s at odds with what happens when hosts produce spike proteins from the RNA of beta-coronaviruses. Two mutations that involve proline substitutions are built in at the beginning of the central helix of the spike protein to force it to stay in its ‘up’ prefusion conformation – the state it’s in before it enters cells, after which it switches to the ‘down’ position. This unnatural ‘up’ position forced upon it by the structurally stiff proline molecules is intended to increase the exposure of the spike protein to the host’s immune system. This way it increases the amount of neutralising antibodies generated through the humoral (adaptive) immune response.
Each mRNA sequence is encased in a nanoparticle comprised of three main components: an ionizable phospholipid (phosphocholine), a sterol and a lipid-anchored polyethylene-glycol (PEG) molecule. This is in effect a targeted drug delivery system that’s never been used at scale before – certainly not in efforts to treat a global population. The lipid nanoparticle (LNP) is multi-functional in that it protects the very fragile mRNA, it reduces particle aggregation and it exploits the tendency of cell membranes to draw the lipid (along with its mRNA cargo) into cells.
It is too early to fully understand how new-to-nature mRNA, modified spike proteins and lipid nanoparticles will affect those injected in the long-term. The likelihood is that these synthetic genetic ‘vaccines’ that are injected directly into our bodies present a substantially greater risk to our species than the consumption of genetically modified foods that has been the subject of open scientific and public discourse for decades, with millions of consumers choosing to avoid their consumption.
Furthermore, it is now well known that the LNPs do not remain in the deltoid muscle injection sites, a fact that was revealed on disclosure of a Japanese biodistribution study used by regulators to grant Emergency Use Authorisation of the Pfizer jab.
The possibility of the mRNA being delivered to a young woman’s ovaries is more than a possibility. If it were to encode for the spike protein, toxicity or an immune response it could adversely affect fertility. It is our view that there is no conclusive evidence that these ‘genetic vaccines’ will not adversely affect fertility of either women or men. This risk is likely to increase with successive exposure to the jabs.
Viral vector type
While these ‘genetic vaccines’ also get the body to produce the spike protein, they are more complex in nature. Unlike RNA jabs that are entirely synthetic in origin, they rely on mammalian cell cultures.
The adenoviral vectors are derived from chimpanzees and are subject to two key mutations: one that eliminates the E1 gene that stops the virus from replicating once in a vaccinee, the other that inserts the DNA of the adenovirus, a cloned gene that encodes for the full-length spike protein.
Source: Heinz FX, Stiasny K. npj Vaccines. 6, 104 (2021)
In the Oxford-AstraZeneca, Gamaleya and CanSino ‘vaccines’, viral vector particles are sourced from primary human foetal kidney cells (HEK293). The Janssen ‘vaccine’ relies on human foetal retinal cells (PER.C6) (Table 2). The process is complex and involves detergents and filters to remove free viral DNA and other debris. On all accounts, some 80% of the overall protein content of the jab may in fact be impurities from the foetal cell lines. Heinz and Stiasny separately calculated that the total protein content of the 50 billion adenoviral vector particles would amount to about 8 micrograms. Yet a separate study found that the actual protein content was much higher, at between 35 to 40 micrograms. This additional amount (80%) must be related to protein-rich cellular impurities from the human foetal cells lines. Have religious groups, vegetarians and vegans been informed of the presence of this human cell line debris?
Instead of the spike protein being made in the cytoplasm and endoplasmic reticulum outside the nucleus of the cell, the viral vectors rely on the adenoviral DNA entering the nucleus and transcribing itself to RNA before it can generate the spike protein. The additional steps mean there are greater possibilities for aberrant genetic processes and transcription patterns, as shown by Almuqrin and colleagues. Animal experiments have shown that the adenoviral DNA, in contrast to mRNA, may remain viable and detectable for months following injection, this being one reason that viral vector jabs are less prone to waning immunity.
Do the ‘vaccines’ contain nanotechnology?
The LNPs in the Pfizer and Moderna jabs certainly are sub-100 nanometres in size. The adenoviral vector types rely on chimp adenoviruses that are typically at or just above this relatively arbitrary threshold. However, given that size really does matter when it comes to changes in biological properties, the lack of robust safety data on the LNP-dependent mRNA jabs is of particular concern.
Equally concerning is that the public keeps being told there’s no nanotechnology in the jabs. Take a quote by Mark Lynas, a visiting fellow at the Alliance for Science and Cornell University, for example. He said, "None of the vaccines contain nanotechnology of any sort, let alone 'transhumanism nanotechnology,’ which isn’t even a thing." Unfortunately, Mark Lynas, who writes for the New York Times, the Washington Post, the Wall Street Journal, the Guardian and CNN.com, is wrong on both counts. As we’ve already seen, the LNPs in the Pfizer and Moderna jabs are most certainly nanoparticles given their size distribution. The game is given away even in their name (LNPs)!
Then there’s the transhumanism claim. It is a thing – potentially a very real thing in the eyes of those who are pushing jabs as the only way out of this ‘pandemic’. For an introduction to transhumanism, you might want to dive into a somewhat conventional take on the subject via Wikipedia. You might also want to check out the Fourth Industrial Revolution (Penguin, 2017), by founder of the World Economic Forum, Klaus Schwab. He describes this as a revolution “characterized by a fusion of technologies that is blurring the lines between the physical, digital, and biological spheres.” Mark Lynas seems unaware of the insights of Schwab and other transhuman proponents on designer beings or humans with gene-edited artificial memories.
To create a robust and durable immune response, you ideally need trained innate immunity coupled with well integrated adaptive immunity made up of an appropriate humoral (B cell derived neutralising antibodies) and cell-mediated (CD4+ and CD8+ T cells) response. Spike protein focused covid-19 jabs largely elevate neutralising antibodies that only partially neutralise the spike protein of the delta variant (even less so for omicron), while damaging both the innate immune and cell-mediated (T cell based) adaptive immune response.
>>> Find out more about how the jabs can interfere with the immune systems of vaccinees
>>> How safe are covid ‘genetic vaccines’?
>>> Pathology conference in Germany (4 December 2021) (with video recording including English voice over) considering adverse effects of covid-19 injections and corruption
>>> Download FDA-released data dump on adverse events from BioNTech/Pfizer (Comirnaty) jab up to 28 Feb 2021
It’s a pandemic of the unvaccinated, right?
The UK Health Security Agency (UK HSA), formerly Public Health England, had a long standing reputation, since the news of a new coronavirus in Wuhan broke in early 2020, as being one of the most comprehensive datasets for epidemiological study.
By October 2021 there was an emerging picture of catastrophic failure of the technology that so much of the industrialised world had appeared to pin its hopes on. That included data from the UK HSA.
It wasn’t long before one of many changes in reporting changed the pattern of the data. Initially it was hard to understand why a process that had looked like increasing ‘vaccine’ failure had suddenly turned itself around, with vaccinees appearing to have better outcomes in terms of cases, hospitalisations and deaths than the jab-free. We started finding anomalies in the data on supposedly covid-caused or all-cause mortality and immediately sensed that what might be going on was that the people who had been initially jabbed were being counted as jab-free.
Then we saw that Dr Martin Neil and Prof Norman Fenton of Queen Mary, University of London, along with a number of other colleagues, had done a stunning analysis of the latest UK HSA data. Don’t expect a major journal to have published the work – as these have all been systematically blocking publication of any scientific views or analysis that contradicts the mainstream narrative. So you’ll have to read the paper, for now at least, on the preprint server Researchgate.
What the researchers found once they’d adjusted all-cause mortalities for likely miscategorisations of deaths was that the jabs had no benefits whatsoever. The first signal that something was wrong came when they saw consistent spikes in all-cause mortality deaths of specific age groups of the jab-free. These coincided with the exact times that jabs were being rolled out to these age groups! How could the jab-free be affected? The answer appears to be: when the reportedly jab-free are actually the jabbed.
Their work is truly disturbing and concludes not only that there was almost certain systemic miscategorisation of deaths between the different categories of unvaccinated and vaccinated, but also delayed or non-reporting of vaccinations, systemic underestimation of the proportion of unvaccinated, and/or incorrect population selection for covid deaths.
It remains to be seen how the UK HSA will respond – but chances are the publication will either be ignored because it was not published in a peer reviewed journal or Dr Neil and Prof Fenton will become targets for abuse and ridicule.
One thing is for sure: the UK HSA can no longer be trusted for its data quality.
Some Numbers
- Over 5.8 million genome sequences of SARS-CoV-2 have been shared with GISAID
- 55% of the world population has received at least one dose of a covid-19 jab
- 21 billion doses have been administered globally
- 87 million are estimated to be administered every day
- Only 6.2% of people in low-income countries have received at least one dose
- Only 7.7% of people in the African continent have received at least one jab
Source: Our World In Data

Figure 1. Covid-19 jab coverage by continent.
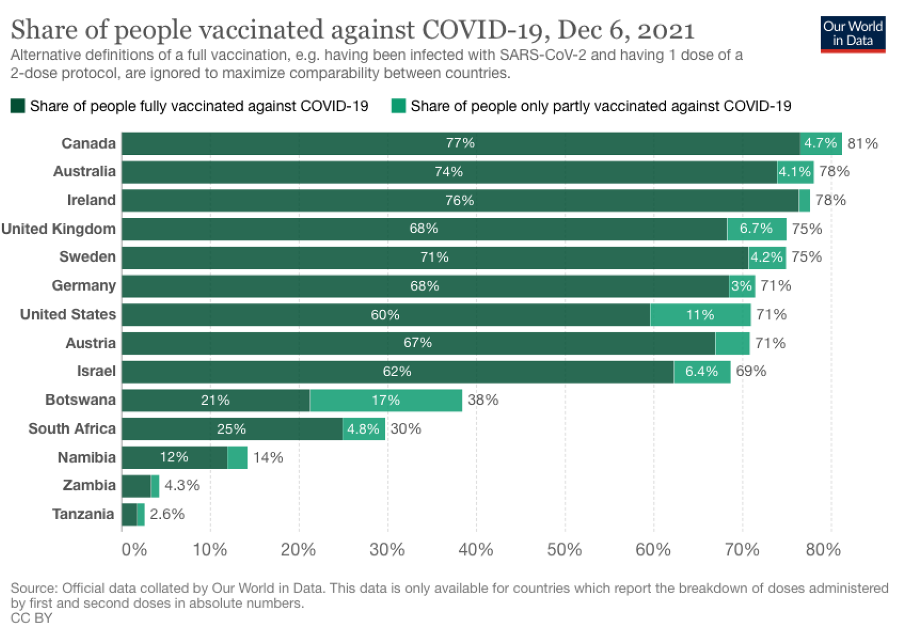
Figure 2. Covid jab coverage in selected countries as of 6 December 2021.
Omicron update
Last week, we published a detailed article on the omicron variant that provided evidence suggesting that it was improbable that the variant originated in southern Africa. We figured it was politically expedient for Africa to be placed under huge pressure to increase its vaccination coverage (see Figs 1 and 2).
Will omicron successfully outcompete delta worldwide? Emerging data from the Tshwane District in South Africa, which has been described as the “global epicentre of Omicron Outbreak”, suggest omicron has been able to outcompete delta in this area and it appears likely this trend will be seen elsewhere.
Final word
This article scrapes the surface of what is known and not known about these gene therapy products widely misrepresented as ‘vaccines’. More than that, misrepresented as ‘safe and effective vaccines’.
Omicron will be used as a lever to jab more people. Recognising that the ‘ardently jab-free’ constitute many of the remaining so-called hesitants, countries like Austria, Germany, Canada and Australia are resorting to mandates or extreme coercion.
European Commission president Ursula von der Leyen has seized the opportunity afforded by omicron to get EU countries to debate and consider mandatory ‘vaccination’ given her concerns over “low vaccination rates” in Europe.
The very least anyone should expect in the face of a virus that is now on par for lethality to circulating flu, is the right to informed consent. That means informing each potential vaccinee what’s in the jabs, what’s known and not known about the greatest experiment ever conducted by, and on, humanity, and what other options there are that are known to effectively combat infection by SARS-CoV-2.
In short, that would mean that nothing you’ve read in this article should come as a surprise to anyone who has been jabbed. And we know from our many discussions, lectures, webinars and conversations around the world over these last 12 or so months, we are a million miles from achieving the required level of understanding for informed medical consent to have been offered.
To help improve the potential for properly informed consent, while allowing others to exercise their right of refusal in those countries that have yet to introduce mandates, please share this article as widely as you can. Thank you.
>>> If you're not already a member, you're very welcome to join our tribe and become an ANH Pathfinder!
>>> For more curated content on the coronavirus crisis visit covidzone.org
>>> Return to the homepage
#enoughmovement #enough




Comments
your voice counts
08 December 2021 at 11:47 pm
Having avoided GMO foods as much as I possibly can, why would I consent to having GMO technology injected into my body?! Some days are harder than others to deal with, today is one of those. Thank you Rob and all the ANHI team for continuing to report the science that I can barely keep up let along understand!
Sue
09 December 2021 at 9:27 am
I do wonder whether your point about informed consent is as clear as it could be.
I believe the UK legal system is based on a combination of statutes which are laws made in parliament and common law which gets updated by legal precedents/judgements made in a court of law.
My understanding is that parliament can't simply ignore judgements or case precedents, otherwise there would be no separation between these various systems and institutions.
In the UK, the laws related to consent changed from Bolam to The Montgomery Ruling.
Here are a couple of articles...
https://www.bmj.com/content/357/bmj.j2224
https://www.themdu.com/guidance-and-advice/guides/montgomery-and-informed-consent
I'm not legally trained, so this needs properly discussing with someone who is better qualified.
When it was suggested I had the Jab, I did ask my doctor a few questions, none of which was answered, so I declined.
What I don't understand is why there don't seem to be any cases challenging the mandated jabs in care homes and in the near future the NHS?
If the government decided to mandate vaccines for all, I do wonder what I would do? Could they certify me as a raving loony and force me?
I would be interested in your feedback.
Thanks
11 December 2021 at 8:41 pm
First off, I want to thank you for writing this wonderful article. It is very detailed. I have included this article in my listing of resources with regards to "vaccine" ingredients.
Secondly, I want to share the following question that I asked at ResearchGate on 26th August 2021 with you and the global audience. I posted 2 PDF documents to that question with information and quotes regarding the "vaccine" ingredients. The link to the question is below:
https://www.researchgate.net/post/Have_any_researchers_taken_samples_from_all_of_the_global_experimental_gene_therapy_injections_to_test_for_any_micro-and_or_nano-contamination
Have any researchers taken samples from all of the global, experimental gene therapy injections to test for any micro- and/or nano-contamination?
Thank you.
08 November 2022 at 9:44 am
To: Irucka Embry, E.I.T. and all others interested.
Re: Studies of Contents of the Experimental Injections
I recommend that you read the following 132-page report on studies of the contents being done internationally. I'll be surprised if anyone, having accepted these poisonous products into their bodies (and not possible substituted placebos), lives anywhere close to their expected lifetime. Search for this, read and weep:
"What is in the so-called COVID-19 'Vaccines'? Part 1: Evidence of a Global Crime Against Humanity" by David A. Hughes, PhD, Senior Lecturer in International Relations, University of Lincoln, Brayford Pool, Lincoln LN6 7TS, England [email protected] .
International Journal of Vaccine Theory, Practice, and Research 2(2), September 3, 2022,
pages 455-586 (=132 pp.) PDF.
Your voice counts
We welcome your comments and are very interested in your point of view, but we ask that you keep them relevant to the article, that they be civil and without commercial links. All comments are moderated prior to being published. We reserve the right to edit or not publish comments that we consider abusive or offensive.
There is extra content here from a third party provider. You will be unable to see this content unless you agree to allow Content Cookies. Cookie Preferences